

Additive effect of aortic regurgitation degree on left ventricular strain in patients with type 2 diabetes mellitus evaluated via cardiac magnetic resonance tissue tracking
- PMID: 35277181
- PMCID: PMC8917654
- DOI: 10.1186/s12933-022-01471-2
Additive effect of aortic regurgitation degree on left ventricular strain in patients with type 2 diabetes mellitus evaluated via cardiac magnetic resonance tissue tracking
Abstract
Background: Type 2 diabetes mellitus causes left ventricular (LV) remodeling and increases the risk of aortic regurgitation (AR), which causes further heart damage. This study aimed to investigate whether AR aggravates LV deformation dysfunction and to identify independent factors affecting the global peak strain (PS) of LV remodeling in patients with type 2 diabetes mellitus (T2DM) who presented with AR and those without T2DM.
Methods: In total, 215 patients with T2DM and 83 age- and sex-matched healthy controls who underwent cardiac magnetic resonance examination were included. Based on the echocardiogram findings, T2DM patients with AR were divided into three groups (mild AR [n = 28], moderate AR [n = 21], and severe AR [n = 17]). LV function and global strain parameters were compared, and multivariate analysis was performed to identify the independent indicators of LV PS.
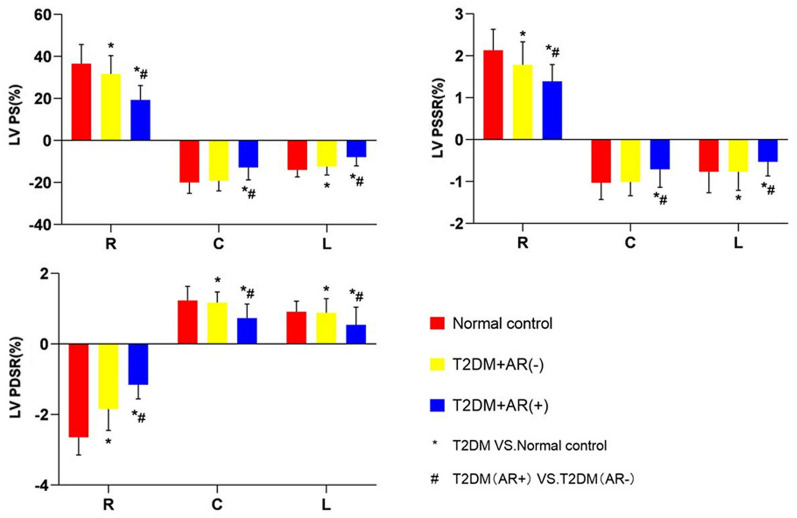
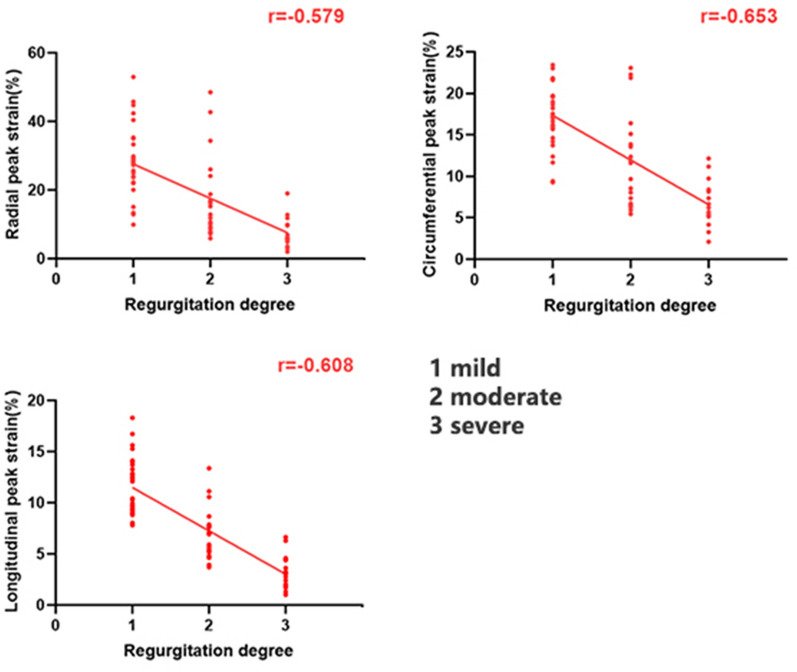
Results: The T2DM patients with AR had a lower LV global PS, peak systolic strain rate (PSSR), and peak diastolic strain rate (PDSR) in three directions than those without AR and non-T2DM controls. Patients without AR had a lower PS (radial and longitudinal) and PDSR in three directions and higher PSSR (radial and longitudinal) than healthy controls. Further, regurgitation degree was an independent factor of LV global radial, circumferential, and longitudinal PS.
Conclusion: AR may aggravate LV stiffness in patients with T2DM, resulting in lower LV strain and function. Regurgitation degree and sex were independently correlated with LV global PS in patients with T2DM and AR.
Keywords: Aortic regurgitation; Left ventricle; Magnetic resonance imaging; Strain; Type 2 diabetes mellitus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Aggravation of functional mitral regurgitation on left ventricle stiffness in type 2 diabetes mellitus patients evaluated by CMR tissue tracking.Cardiovasc Diabetol. 2021 Jul 31;20(1):158. doi: 10.1186/s12933-021-01354-y. Cardiovasc Diabetol. 2021. PMID: 34332579 Free PMC article.
-
The adverse impact of coronary artery disease on left ventricle systolic and diastolic function in patients with type 2 diabetes mellitus: a 3.0T CMR study.Cardiovasc Diabetol. 2022 Feb 22;21(1):30. doi: 10.1186/s12933-022-01467-y. Cardiovasc Diabetol. 2022. PMID: 35193565 Free PMC article.
-
Impact of type 2 diabetes mellitus on left ventricular deformation in non-ischemic dilated cardiomyopathy patients assessed by cardiac magnetic resonance imaging.Cardiovasc Diabetol. 2022 Jun 4;21(1):94. doi: 10.1186/s12933-022-01533-5. Cardiovasc Diabetol. 2022. PMID: 35659302 Free PMC article.
-
Noninvasive Imaging for Native Aortic Valve Regurgitation.J Am Soc Echocardiogr. 2024 Dec;37(12):1167-1181. doi: 10.1016/j.echo.2024.08.009. Epub 2024 Aug 30. J Am Soc Echocardiogr. 2024. PMID: 39218370 Review.
-
Aortic Regurgitation: Review of Current Management.Dimens Crit Care Nurs. 2024 Mar-Apr 01;43(2):80-86. doi: 10.1097/DCC.0000000000000628. Dimens Crit Care Nurs. 2024. PMID: 38271313 Review.
Cited by
-
Additive effects of mitral regurgitation on left ventricular strain in essential hypertensive patients as evaluated by cardiac magnetic resonance feature tracking.Front Cardiovasc Med. 2022 Nov 10;9:995366. doi: 10.3389/fcvm.2022.995366. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36440008 Free PMC article.
-
A multicenter study on the comparability of myocardial strain values acquired with different CMR scanners and analyzed with different post-processing software: insights into the "Traveling Volunteers" study.Int J Comput Assist Radiol Surg. 2025 Aug 30. doi: 10.1007/s11548-025-03499-7. Online ahead of print. Int J Comput Assist Radiol Surg. 2025. PMID: 40884734
-
Evaluation of left ventricular systolic function in type 2 diabetes mellitus patients with and without peripheral vascular disease.World J Diabetes. 2024 Jun 15;15(6):1280-1290. doi: 10.4239/wjd.v15.i6.1280. World J Diabetes. 2024. PMID: 38983825 Free PMC article.
-
Association of abdominal adiposity, hepatic shear stiffness with subclinical left-ventricular remodeling evaluated by magnetic resonance in adults free of overt cardiovascular diseases: a prospective study.Cardiovasc Diabetol. 2023 Apr 29;22(1):99. doi: 10.1186/s12933-023-01828-1. Cardiovasc Diabetol. 2023. PMID: 37120545 Free PMC article.
-
Impact of diabetes mellitus on myocardial function and clinical outcomes in patients with significant aortic regurgitation.Cardiovasc Diabetol. 2025 Jul 15;24(1):290. doi: 10.1186/s12933-025-02843-0. Cardiovasc Diabetol. 2025. PMID: 40665315 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
