

Phase 2 trial of T-cell activation using MVI-816 and pembrolizumab in patients with metastatic, castration-resistant prostate cancer (mCRPC)
- PMID: 35277461
- PMCID: PMC8919462
- DOI: 10.1136/jitc-2021-004198
Phase 2 trial of T-cell activation using MVI-816 and pembrolizumab in patients with metastatic, castration-resistant prostate cancer (mCRPC)
Abstract
Background: We previously reported a trial using a DNA vaccine encoding prostatic acid phosphatase (MVI-816, pTVG-HP), given over 12 weeks concurrently or sequentially with pembrolizumab, in patients with mCRPC. We report the final analysis of this trial following two additional treatment arms in which patients with mCRPC continued concurrent treatment until progression.
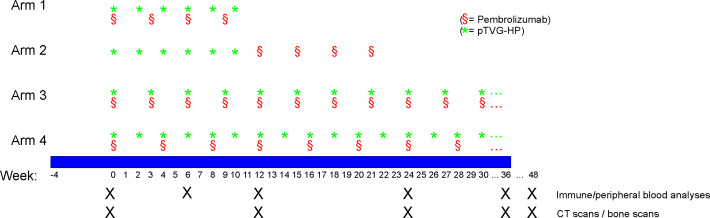
Materials and methods: Patients with mCRPC were treated with MVI-816 and pembrolizumab every 3 weeks (arm 3, n=20) or MVI-816 every 2 weeks and pembrolizumab every 4 weeks (arm 4, n=20). The primary objectives were safety, 6-month progression-free survival (PFS), median time to radiographic progression, and objective response rates. Secondary objectives included immunological evaluations.
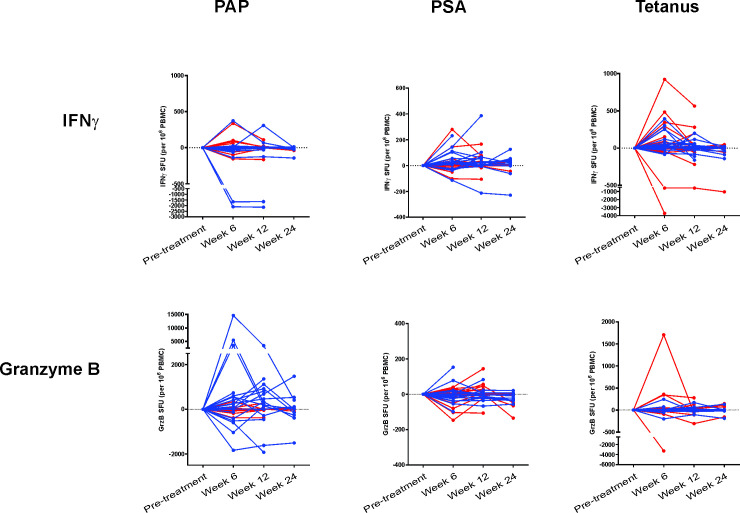
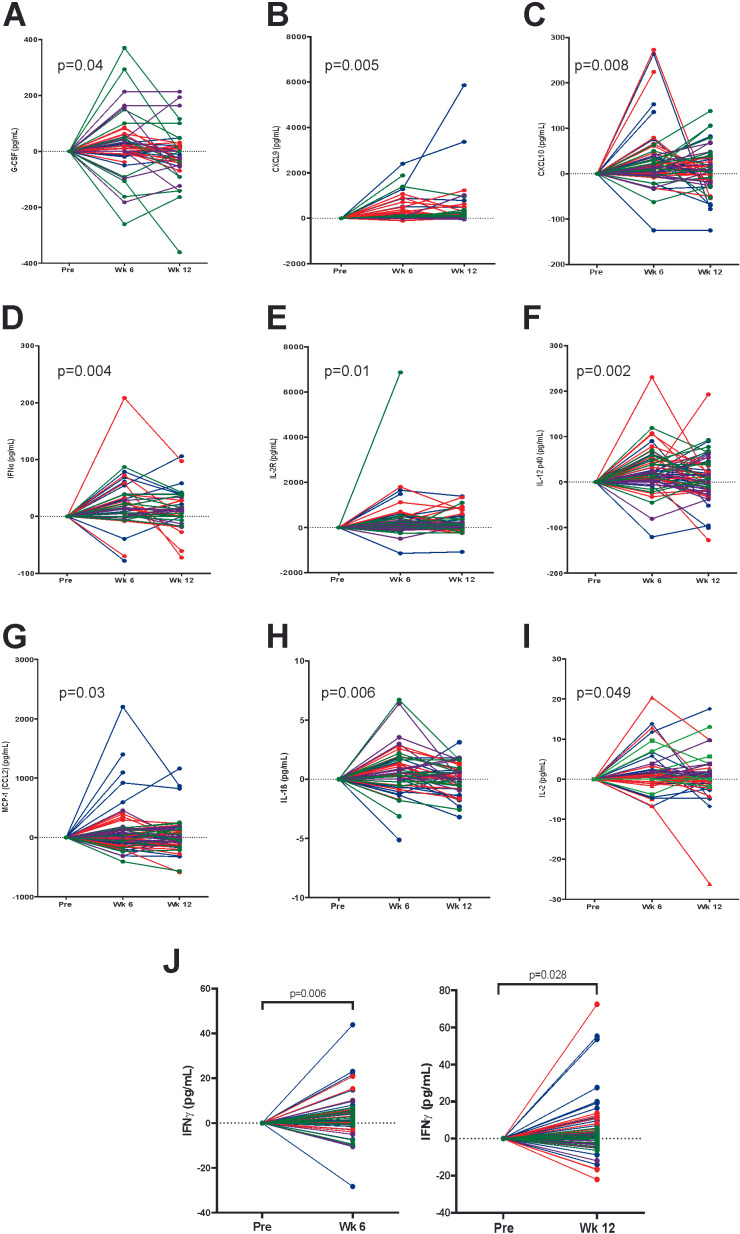
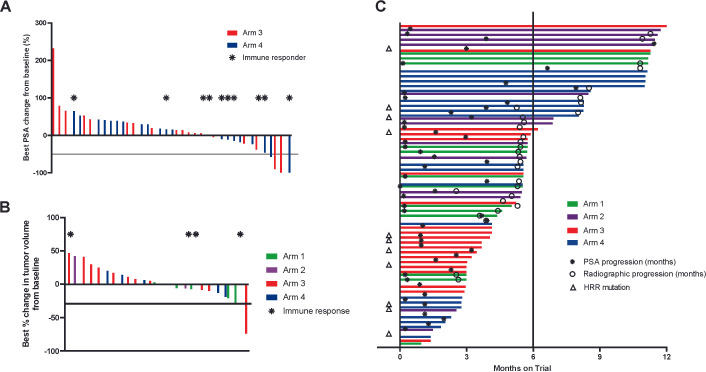
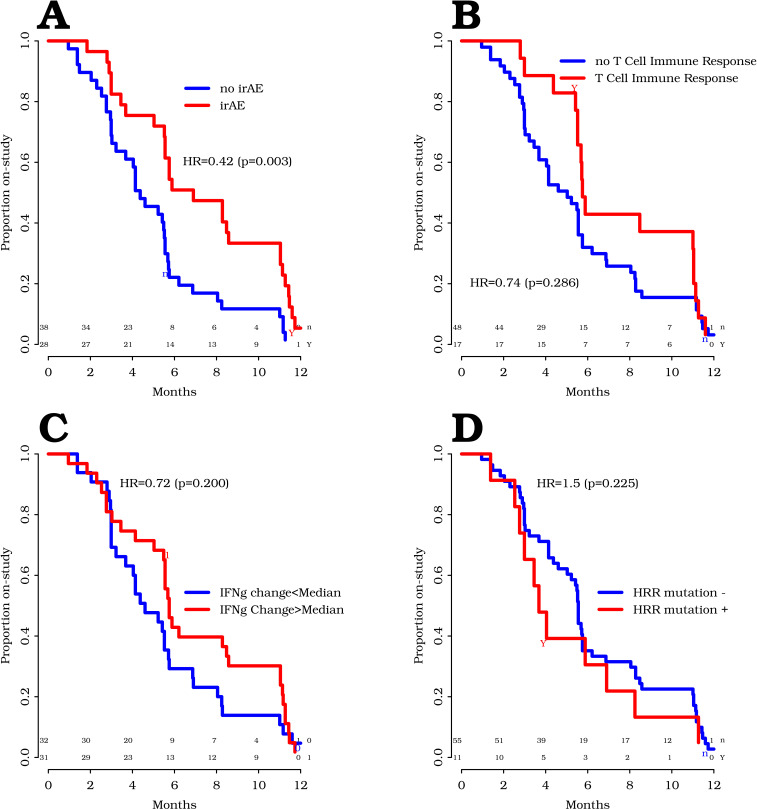
Results: In 25 patients with measurable disease, there were no complete response and one confirmed partial response in a patient who subsequently found to have an MSIhi tumor. 4/40 patients (10%) had a prostate-specific antigen decline >50%. The estimated overall radiographic PFS rate at 6 months was 47.2% (44.4% arm 3, 61.5% arm 4). Accounting for all off-study events, overall median time on treatment was 5.6 months (95% CI: 5.4 to 10.8 months), 5.6 months for arm 3 and 8.1 months for arm 4 (p=0.64). Thirty-two per cent of patients remained on trial beyond 6 months without progression. Median overall survival was 22.9 (95% CI: 16.2 to 25.6) months. One grade 4 event (hyperglycemia) was observed. Immune-related adverse events (irAEs) >grade 1 were observed in 42% of patients overall. Interferon-γ and/or granzyme B immune response to prostatic acid phosphatase was detected in 2/20 patients in arm 3 and 6/20 patients in arm 4. Plasma cytokines associated with immune activation and CD8+ T-cell recruitment were augmented at weeks 6 and 12. The development of irAE was significantly associated with a prolonged time on treatment (HR=0.42, p=0.003). Baseline DNA homologous recombination repair mutations were not associated with longer time to progression.
Conclusions: Findings here demonstrate that combining programmed cell death 1 blockade with MVI-816 is safe, can augment tumor-specific T cells, and can result in a favorable 6-month disease control rate. Correlative studies suggest T-cell activation by vaccination is critical to the mechanism of action of this combination. Future randomized clinical trials are needed to validate these findings.
Trial registration number: NCT02499835.
Keywords: clinical trials, phase II as topic; costimulatory and inhibitory T-cell receptors; immunogenicity, vaccine; prostatic neoplasms.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DGM has ownership interest, has received research support, and serves as consultant to Madison Vaccines, which has licensed material described in this manuscript and supported this trial.
Figures
Similar articles
-
Phase 2 trial of a DNA vaccine (pTVG-HP) and nivolumab in patients with castration-sensitive non-metastatic (M0) prostate cancer.J Immunother Cancer. 2023 Dec 14;11(12):e008067. doi: 10.1136/jitc-2023-008067. J Immunother Cancer. 2023. PMID: 38101860 Free PMC article. Clinical Trial.
-
Prime-boost vaccination targeting prostatic acid phosphatase (PAP) in patients with metastatic castration-resistant prostate cancer (mCRPC) using Sipuleucel-T and a DNA vaccine.J Immunother Cancer. 2018 Mar 13;6(1):21. doi: 10.1186/s40425-018-0333-y. J Immunother Cancer. 2018. PMID: 29534736 Free PMC article. Clinical Trial.
-
Phase II Trial of a DNA Vaccine Encoding Prostatic Acid Phosphatase (pTVG-HP [MVI-816]) in Patients With Progressive, Nonmetastatic, Castration-Sensitive Prostate Cancer.J Clin Oncol. 2019 Dec 20;37(36):3507-3517. doi: 10.1200/JCO.19.01701. Epub 2019 Oct 23. J Clin Oncol. 2019. PMID: 31644357 Free PMC article. Clinical Trial.
-
A phase II single-arm study of pembrolizumab with enzalutamide in men with metastatic castration-resistant prostate cancer progressing on enzalutamide alone.J Immunother Cancer. 2020 Jul;8(2):e000642. doi: 10.1136/jitc-2020-000642. J Immunother Cancer. 2020. PMID: 32616555 Free PMC article. Clinical Trial.
-
Pembrolizumab for Previously Treated Advanced or Metastatic Urothelial Cancer: An Evidence Review Group Perspective of a NICE Single Technology Appraisal.Pharmacoeconomics. 2019 Jan;37(1):19-27. doi: 10.1007/s40273-018-0689-3. Pharmacoeconomics. 2019. PMID: 30030817 Review.
Cited by
-
The application of emerging immunotherapy in the treatment of prostate cancer: progress, dilemma and promise.Front Immunol. 2025 Mar 12;16:1544882. doi: 10.3389/fimmu.2025.1544882. eCollection 2025. Front Immunol. 2025. PMID: 40145100 Free PMC article. Review.
-
Long-term follow up of patients treated with a DNA vaccine (pTVG-hp) for PSA-recurrent prostate cancer.Hum Vaccin Immunother. 2024 Dec 31;20(1):2395680. doi: 10.1080/21645515.2024.2395680. Epub 2024 Aug 29. Hum Vaccin Immunother. 2024. PMID: 39208856 Free PMC article. Clinical Trial.
-
Phase 2 trial of a DNA vaccine (pTVG-HP) and nivolumab in patients with castration-sensitive non-metastatic (M0) prostate cancer.J Immunother Cancer. 2023 Dec 14;11(12):e008067. doi: 10.1136/jitc-2023-008067. J Immunother Cancer. 2023. PMID: 38101860 Free PMC article. Clinical Trial.
-
Prostate cancer immunotherapy: a review of recent advancements with novel treatment methods and efficacy.Am J Clin Exp Urol. 2022 Aug 15;10(4):210-233. eCollection 2022. Am J Clin Exp Urol. 2022. PMID: 36051616 Free PMC article. Review.
-
Targeted Radiation and Immune Therapies-Advances and Opportunities for the Treatment of Prostate Cancer.Pharmaceutics. 2023 Jan 11;15(1):252. doi: 10.3390/pharmaceutics15010252. Pharmaceutics. 2023. PMID: 36678880 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous