

Searching for optimal machine learning model to classify mild cognitive impairment (MCI) subtypes using multimodal MRI data
- PMID: 35277565
- PMCID: PMC8917197
- DOI: 10.1038/s41598-022-08231-y
Searching for optimal machine learning model to classify mild cognitive impairment (MCI) subtypes using multimodal MRI data
Abstract
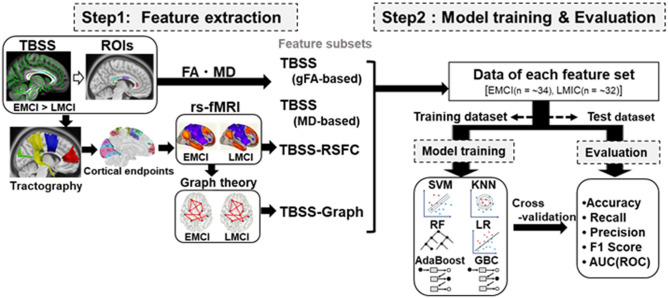
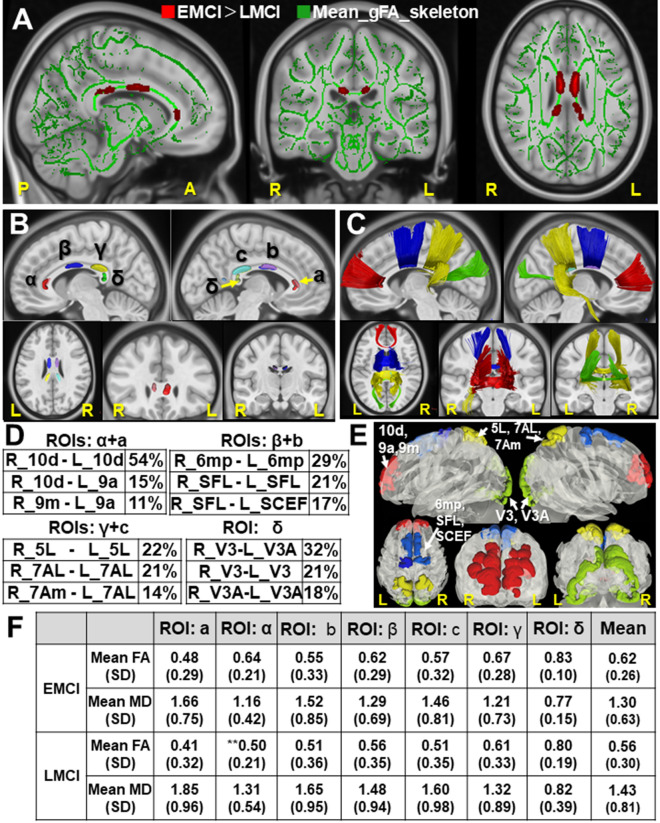
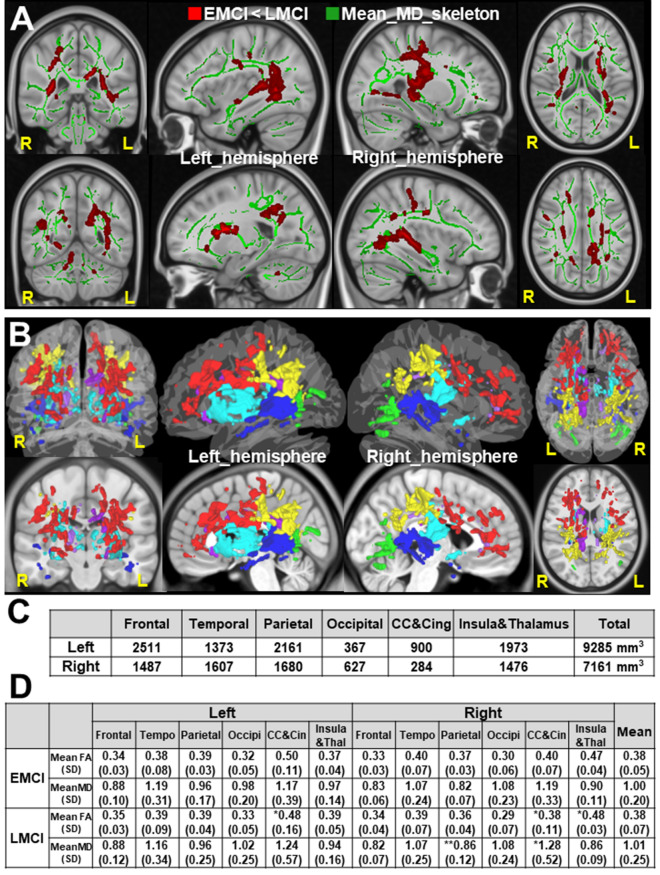
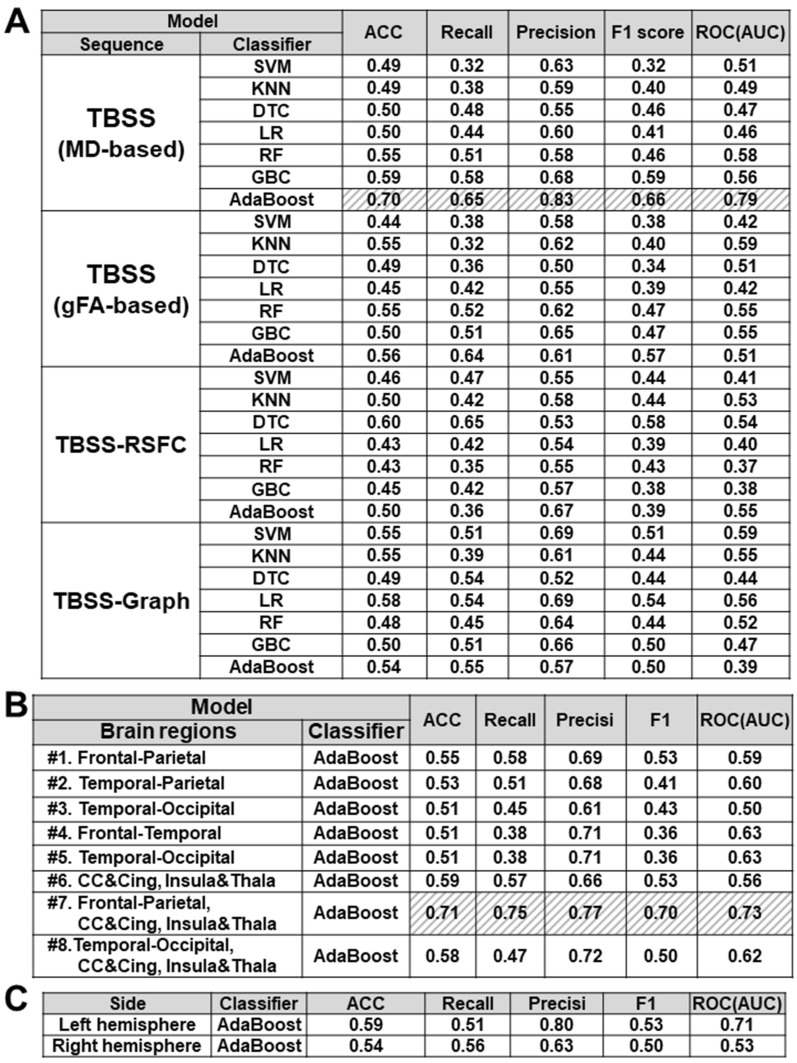
The intervention at the stage of mild cognitive impairment (MCI) is promising for preventing Alzheimer's disease (AD). This study aims to search for the optimal machine learning (ML) model to classify early and late MCI (EMCI and LMCI) subtypes using multimodal MRI data. First, the tract-based spatial statistics (TBSS) analyses showed LMCI-related white matter changes in the Corpus Callosum. The ROI-based tractography addressed the connected cortical areas by affected callosal fibers. We then prepared two feature subsets for ML by measuring resting-state functional connectivity (TBSS-RSFC method) and graph theory metrics (TBSS-Graph method) in these cortical areas, respectively. We also prepared feature subsets of diffusion parameters in the regions of LMCI-related white matter alterations detected by TBSS analyses. Using these feature subsets, we trained and tested multiple ML models for EMCI/LMCI classification with cross-validation. Our results showed the ensemble ML model (AdaBoost) with feature subset of diffusion parameters achieved better performance of mean accuracy 70%. The useful brain regions for classification were those, including frontal, parietal lobe, Corpus Callosum, cingulate regions, insula, and thalamus regions. Our findings indicated the optimal ML model using diffusion parameters might be effective to distinguish LMCI from EMCI subjects at the prodromal stage of AD.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Morris JC, et al. Mild cognitive impairment represents early-stage Alzheimer disease. Arch. Neurol. 2001;58:397–405. - PubMed
-
- Alzheimer’s Disease Facts and Figures Alzheimers dement. J. Alzheimers Assoc. 2021;17:327–406. - PubMed
-
- Jessen F, et al. AD dementia risk in late MCI, in early MCI, and in subjective memory impairment. Alzheimers Dement. J. Alzheimers Assoc. 2014;10:76–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
