

Advances in local therapy for glioblastoma - taking the fight to the tumour
- PMID: 35277681
- PMCID: PMC10359969
- DOI: 10.1038/s41582-022-00621-0
Advances in local therapy for glioblastoma - taking the fight to the tumour
Abstract
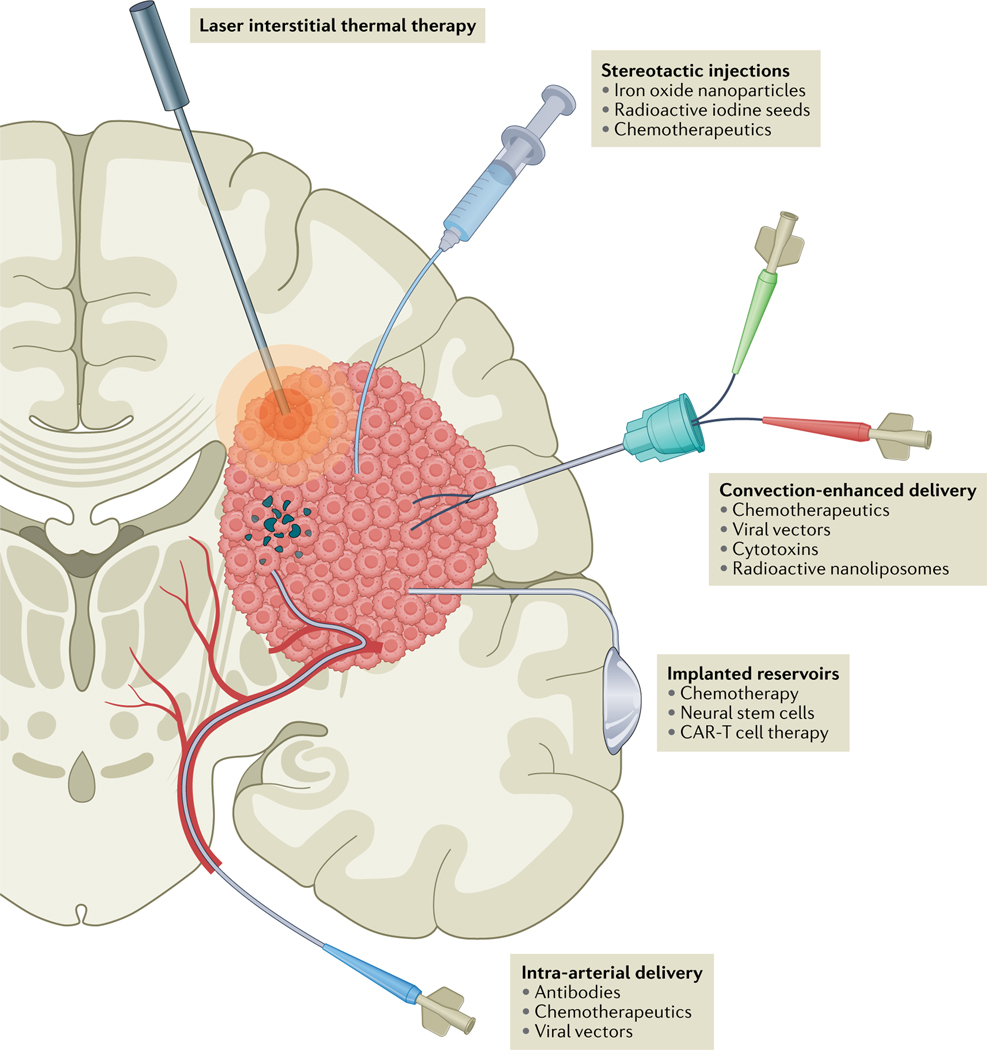
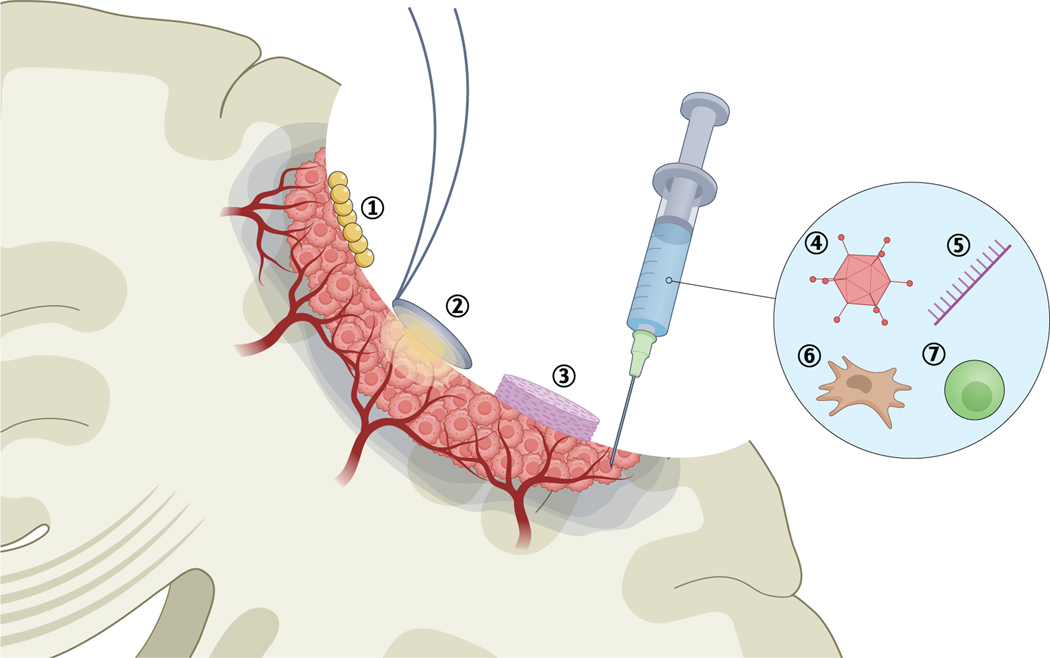
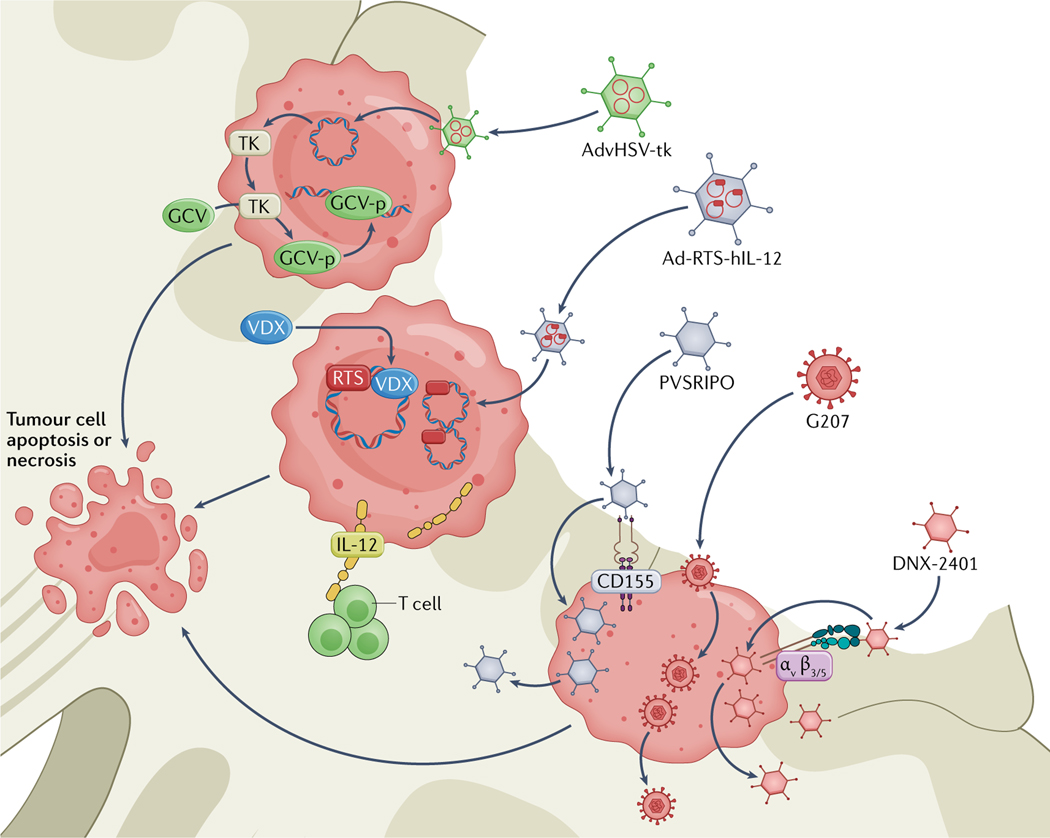
Despite advances in neurosurgery, chemotherapy and radiotherapy, glioblastoma remains one of the most treatment-resistant CNS malignancies, and the tumour inevitably recurs. The majority of recurrences appear in or near the resection cavity, usually within the area that received the highest dose of radiation. Many new therapies focus on combatting these local recurrences by implementing treatments directly in or near the tumour bed. In this Review, we discuss the latest developments in local therapy for glioblastoma, focusing on recent preclinical and clinical trials. The approaches that we discuss include novel intraoperative techniques, various treatments of the surgical cavity, stereotactic injections directly into the tumour, and new developments in convection-enhanced delivery and intra-arterial treatments.
© 2022. Springer Nature Limited.
Conflict of interest statement
Competing interests
E.A.C. is currently an advisor to Advantagene, Alcyone Biosciences, Insightec, DNAtrix, Immunomic Therapeutics, Seneca Therapeutics, GlaxoSmithKline and Voyager Therapeutics and has equity interest in DNAtrix, Immunomic Therapeutics and Seneca Therapeutics; he has also advised Oncorus, Merck, Tocagen, Ziopharm, Stemgen, NanoTx., Ziopharm Oncology, Cerebral Therapeutics, Genenta. Merck, Janssen, Karcinolysis, Shanghai Biotech and Sangamo Therapeutics. He has received research support from the NIH, the US Department of Defense, the American Brain Tumor Association, the National Brain Tumor Society, the Alliance for Cancer Gene Therapy, the Neurosurgical Research Education Foundation, Advantagene, NewLink Genetics and Amgen. He is also a named inventor on patents related to oncolytic HSV-1 and non-coding RNAs. The other authors declare no competing interests.
Figures
References
-
- Stupp R. et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med 352, 987–996 (2005). - PubMed
-
- Stupp R. et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 10, 459–466 (2009). - PubMed
-
- Stupp R. et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: a randomized clinical trial. JAMA 314, 2535–2543 (2015). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
