

Interactions among common non-SARS-CoV-2 respiratory viruses and influence of the COVID-19 pandemic on their circulation in New York City
- PMID: 35278037
- PMCID: PMC9111828
- DOI: 10.1111/irv.12976
Interactions among common non-SARS-CoV-2 respiratory viruses and influence of the COVID-19 pandemic on their circulation in New York City
Abstract
Background: Non-pharmaceutical interventions (NPIs) and voluntary behavioral changes during the COVID-19 pandemic have influenced the circulation of non-SARS-CoV-2 respiratory infections. We aimed to examine interactions among common non-SARS-CoV-2 respiratory virus and further estimate the impact of the COVID-19 pandemic on these viruses.
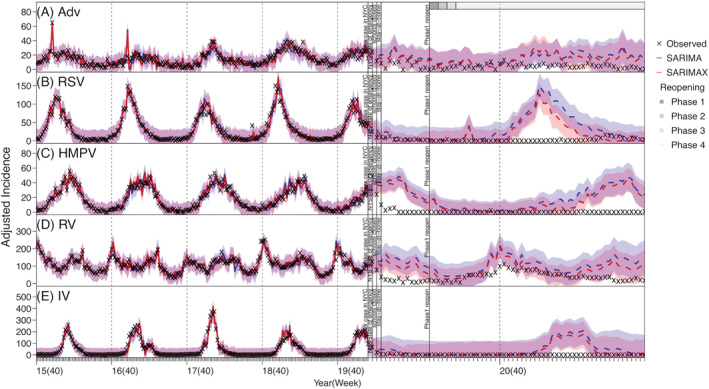
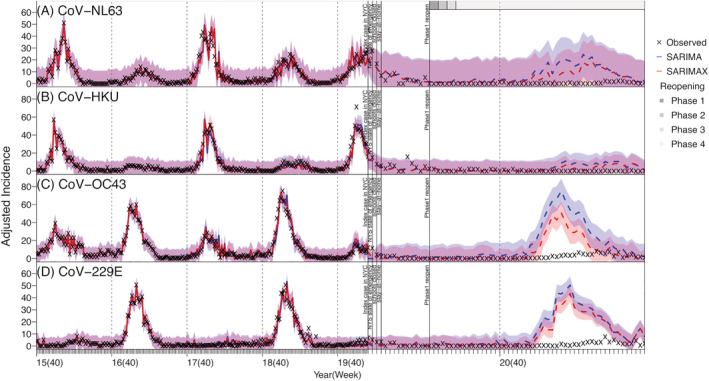
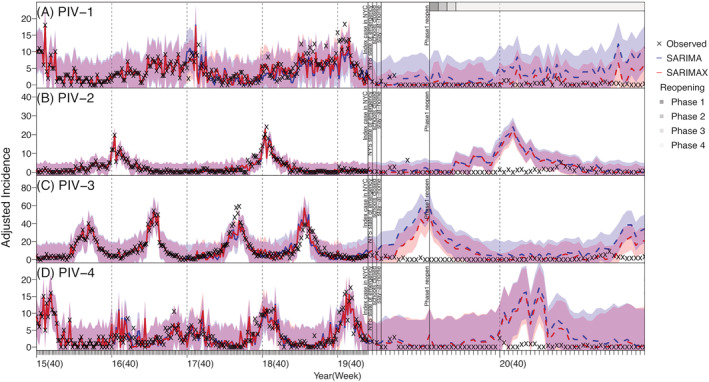
Methods: We analyzed incidence data for seven groups of respiratory viruses in New York City (NYC) during October 2015 to May 2021 (i.e., before and during the COVID-19 pandemic). We first used elastic net regression to identify potential virus interactions and further examined the robustness of the found interactions by comparing the performance of Seasonal Auto Regressive Integrated Moving Average (SARIMA) models with and without the interactions. We then used the models to compute counterfactual estimates of cumulative incidence and estimate the reduction during the COVID-19 pandemic period from March 2020 to May 2021, for each virus.
Results: We identified potential interactions for three endemic human coronaviruses (CoV-NL63, CoV-HKU, and CoV-OC43), parainfluenza (PIV)-1, rhinovirus, and respiratory syncytial virus (RSV). We found significant reductions (by ~70-90%) in cumulative incidence of CoV-OC43, CoV-229E, human metapneumovirus, PIV-2, PIV-4, RSV, and influenza virus during the COVID-19 pandemic. In contrast, the circulation of adenovirus and rhinovirus was less affected.
Conclusions: Circulation of several respiratory viruses has been low during the COVID-19 pandemic, which may lead to increased population susceptibility. It is thus important to enhance monitoring of these viruses and promptly enact measures to mitigate their health impacts (e.g., influenza vaccination campaign and hospital infection prevention) as societies resume normal activities.
Keywords: COVID-19 pandemic impact; coronaviruses; human metapneumovirus; parainfluenza; respiratory virus interactions; rhinovirus.
© 2022 The Authors. Influenza and Other Respiratory Viruses published by John Wiley & Sons Ltd.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
