

Incidence, clinical associations and outcomes of intrathoracic complications with and without ARDS in COVID-19 pneumonia
- PMID: 35278869
- PMCID: PMC8895681
- DOI: 10.1016/j.clinimag.2022.02.029
Incidence, clinical associations and outcomes of intrathoracic complications with and without ARDS in COVID-19 pneumonia
Abstract
Purpose: To determine the incidence and clinical predictors of intrathoracic complications in COVID-19 patients, and the association with outcomes.
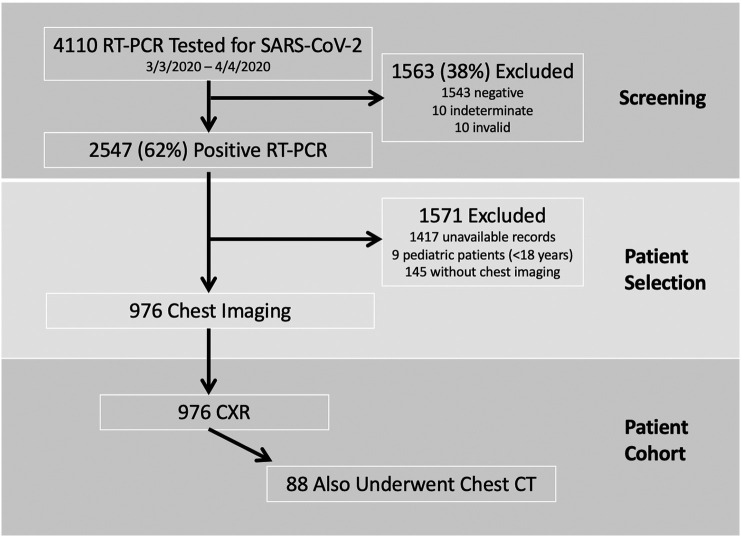
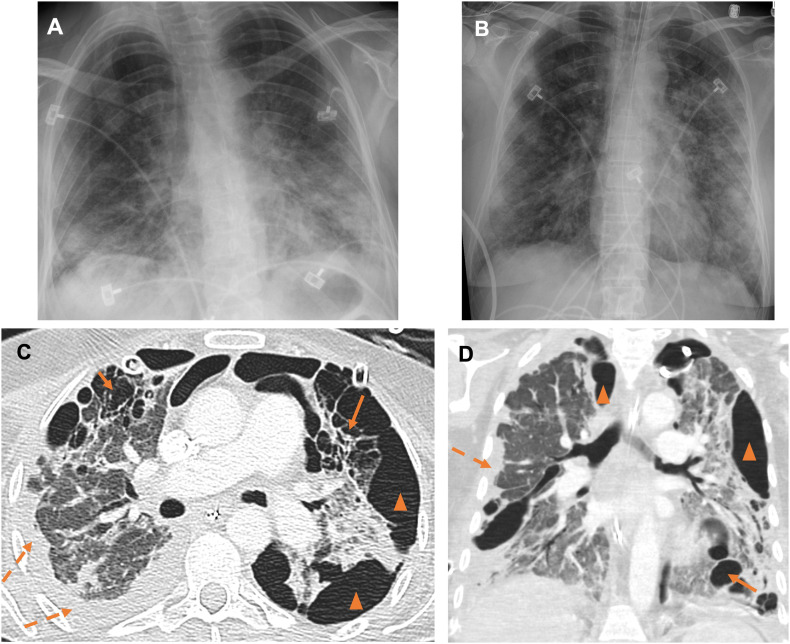
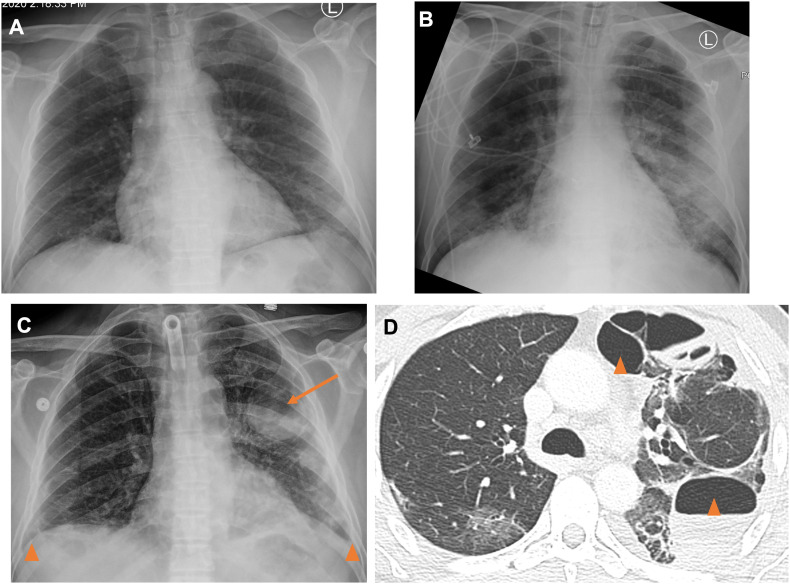
Methods: In this retrospective cross-sectional study, we included 976 patients (age 61 ± 17 years, 62% male) who tested positive for SARS-CoV-2 between March 3-April 4, 2020 and underwent chest imaging. 3836 radiographs from 976 patients and 105 CTs from 88 patients were reviewed for intrathoracic complications, including pneumothorax, pneumomediastinum, pneumopericardium, lobar collapse, pleural effusion, and pneumatocele formation.
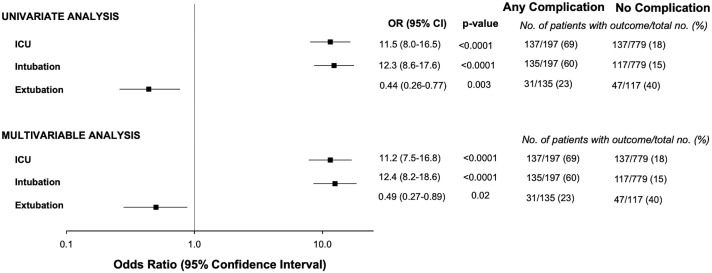
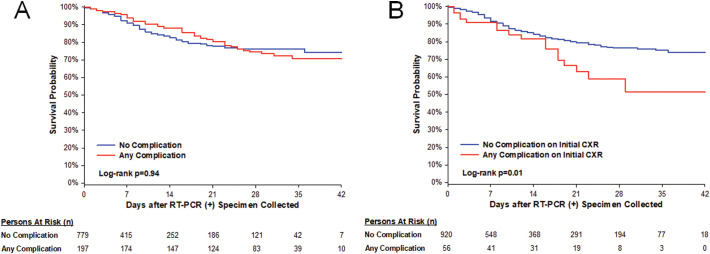
Results: There was a high rate of intrathoracic complications (197/976, 20%). Pleural effusion was the most common complication (168/976, 17%). Pneumothorax (30/976, 3%) and pneumatoceles (9/88, 10%) were also frequent. History of hypertension and high initial CXR severity score were independent risk factors for complications. Patients with any intrathoracic complication during admission had an over 11-fold risk of ICU admission (adjusted odds ratio [aOR] 11.2, p < 0.0001) and intubation (aOR 12.4, p < 0.0001), over 50% reduction in successful extubation (aOR 0.49, p = 0.02) and longer length of stay (median 13 versus 5 days, p < 0.0001). There was no difference in overall survival between patients with and without any complication (log-rank p = 0.94).
Conclusion: In COVID-19 patients who underwent chest imaging, 1 in 5 patients have an intrathoracic complication, which are associated with higher level of care and prolonged hospital stay. Hypertension history and high CXR severity score confer an increased risk of complication.
Summary: Intrathoracic complications in COVID-19 are common and are predictive of ICU admission, need for intubation, less successful extubation, and longer length of stay but are not predictive of mortality.
Keywords: COVID-19; Intubation; Length of stay; Pneumothorax; SARS-CoV-2.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Metabolic Syndrome and Acute Respiratory Distress Syndrome in Hospitalized Patients With COVID-19.JAMA Netw Open. 2021 Dec 1;4(12):e2140568. doi: 10.1001/jamanetworkopen.2021.40568. JAMA Netw Open. 2021. PMID: 34935924 Free PMC article.
-
Serious complications in COVID-19 ARDS cases: pneumothorax, pneumomediastinum, subcutaneous emphysema and haemothorax.Epidemiol Infect. 2021 Jun 8;149:e137. doi: 10.1017/S0950268821001291. Epidemiol Infect. 2021. PMID: 34099076 Free PMC article.
-
The analysis of pleural complications of COVID-19 pneumonia.Turk J Med Sci. 2021 Dec 13;51(6):2822-2826. doi: 10.3906/sag-2012-268. Turk J Med Sci. 2021. PMID: 33890447 Free PMC article.
-
Limitation of tube thoracostomy in treating pneumothorax in COVID-19 infected patients. A retrospective cohort study.Ann Med Surg (Lond). 2022 Aug;80:104171. doi: 10.1016/j.amsu.2022.104171. Epub 2022 Jul 18. Ann Med Surg (Lond). 2022. PMID: 35875057 Free PMC article.
-
Alveolar Air Leak Syndrome a Potential Complication of COVID- 19-ARDS - Single Center Retrospective Analysis.J Assoc Physicians India. 2021 Jan;69(1):22-26. J Assoc Physicians India. 2021. PMID: 34227771 Review.
Cited by
-
Evolution of SARS-CoV-2 related pneumatoceles: A case report.Respir Med Case Rep. 2024 Apr 27;49:102027. doi: 10.1016/j.rmcr.2024.102027. eCollection 2024. Respir Med Case Rep. 2024. PMID: 38737834 Free PMC article.
-
Pleural Effusion in COVID-19 Pneumonia: Clinical and Prognostic Implications-An Observational, Retrospective Study.J Clin Med. 2023 Jan 29;12(3):1049. doi: 10.3390/jcm12031049. J Clin Med. 2023. PMID: 36769697 Free PMC article.
-
Macklin effect on baseline chest CT scan accurately predicts barotrauma in COVID-19 patients.Respir Med. 2022 Jun;197:106853. doi: 10.1016/j.rmed.2022.106853. Epub 2022 Apr 20. Respir Med. 2022. PMID: 35512457 Free PMC article.
References
-
- Hosseiny M., Kooraki S., Gholamrezanezhad A., Reddy S., Myers L. Radiology perspective of coronavirus disease 2019 (COVID-19): lessons from severe acute respiratory syndrome and Middle East respiratory syndrome. AJR Am J Roentgenol. 05 2020;214(5):1078–1082. doi: 10.2214/AJR.20.22969. - DOI - PubMed
-
- Ozsoy I.E., Tezcan M.A., Guzeldag S., Ozdemir A.T. Is spontaneous pneumomediastinum a poor prognostic factor in Covid-19? J Coll Physicians Surg Pak. 2021 Feb;31(2):132–137. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
