

Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020-21
- PMID: 35279232
- PMCID: PMC8912932
- DOI: 10.1016/S0140-6736(21)02796-3
Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020-21
Erratum in
-
Department of Error.Lancet. 2022 Apr 16;399(10334):1468. doi: 10.1016/S0140-6736(22)00621-3. Lancet. 2022. PMID: 35430019 Free PMC article. No abstract available.
Abstract
Background: Mortality statistics are fundamental to public health decision making. Mortality varies by time and location, and its measurement is affected by well known biases that have been exacerbated during the COVID-19 pandemic. This paper aims to estimate excess mortality from the COVID-19 pandemic in 191 countries and territories, and 252 subnational units for selected countries, from Jan 1, 2020, to Dec 31, 2021.
Methods: All-cause mortality reports were collected for 74 countries and territories and 266 subnational locations (including 31 locations in low-income and middle-income countries) that had reported either weekly or monthly deaths from all causes during the pandemic in 2020 and 2021, and for up to 11 year previously. In addition, we obtained excess mortality data for 12 states in India. Excess mortality over time was calculated as observed mortality, after excluding data from periods affected by late registration and anomalies such as heat waves, minus expected mortality. Six models were used to estimate expected mortality; final estimates of expected mortality were based on an ensemble of these models. Ensemble weights were based on root mean squared errors derived from an out-of-sample predictive validity test. As mortality records are incomplete worldwide, we built a statistical model that predicted the excess mortality rate for locations and periods where all-cause mortality data were not available. We used least absolute shrinkage and selection operator (LASSO) regression as a variable selection mechanism and selected 15 covariates, including both covariates pertaining to the COVID-19 pandemic, such as seroprevalence, and to background population health metrics, such as the Healthcare Access and Quality Index, with direction of effects on excess mortality concordant with a meta-analysis by the US Centers for Disease Control and Prevention. With the selected best model, we ran a prediction process using 100 draws for each covariate and 100 draws of estimated coefficients and residuals, estimated from the regressions run at the draw level using draw-level input data on both excess mortality and covariates. Mean values and 95% uncertainty intervals were then generated at national, regional, and global levels. Out-of-sample predictive validity testing was done on the basis of our final model specification.
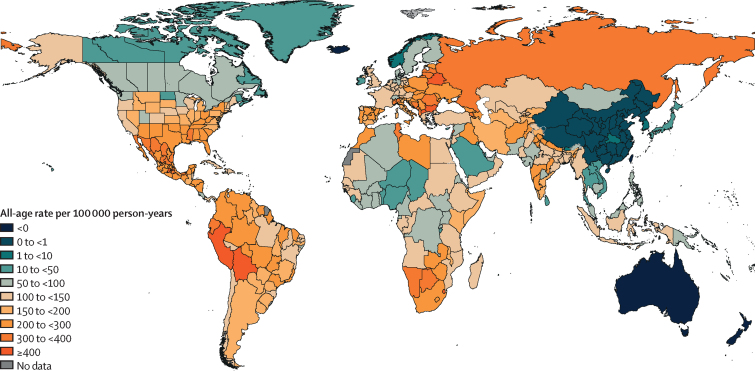
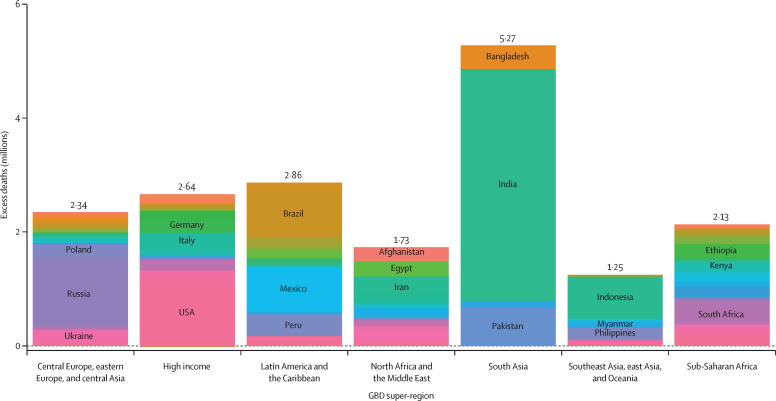
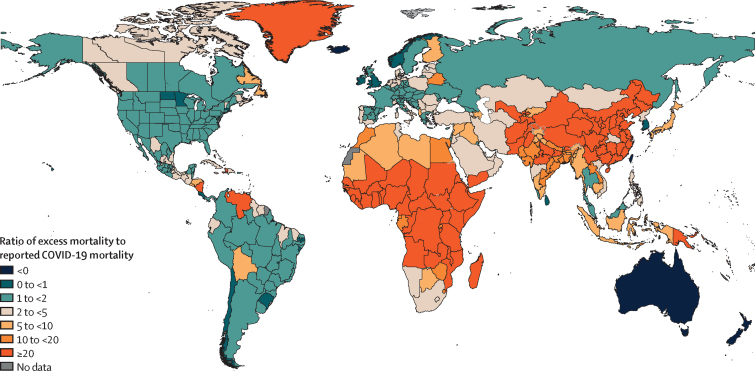
Findings: Although reported COVID-19 deaths between Jan 1, 2020, and Dec 31, 2021, totalled 5·94 million worldwide, we estimate that 18·2 million (95% uncertainty interval 17·1-19·6) people died worldwide because of the COVID-19 pandemic (as measured by excess mortality) over that period. The global all-age rate of excess mortality due to the COVID-19 pandemic was 120·3 deaths (113·1-129·3) per 100 000 of the population, and excess mortality rate exceeded 300 deaths per 100 000 of the population in 21 countries. The number of excess deaths due to COVID-19 was largest in the regions of south Asia, north Africa and the Middle East, and eastern Europe. At the country level, the highest numbers of cumulative excess deaths due to COVID-19 were estimated in India (4·07 million [3·71-4·36]), the USA (1·13 million [1·08-1·18]), Russia (1·07 million [1·06-1·08]), Mexico (798 000 [741 000-867 000]), Brazil (792 000 [730 000-847 000]), Indonesia (736 000 [594 000-955 000]), and Pakistan (664 000 [498 000-847 000]). Among these countries, the excess mortality rate was highest in Russia (374·6 deaths [369·7-378·4] per 100 000) and Mexico (325·1 [301·6-353·3] per 100 000), and was similar in Brazil (186·9 [172·2-199·8] per 100 000) and the USA (179·3 [170·7-187·5] per 100 000).
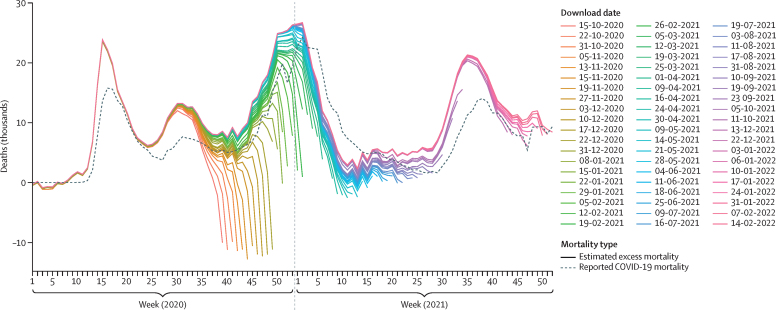
Interpretation: The full impact of the pandemic has been much greater than what is indicated by reported deaths due to COVID-19 alone. Strengthening death registration systems around the world, long understood to be crucial to global public health strategy, is necessary for improved monitoring of this pandemic and future pandemics. In addition, further research is warranted to help distinguish the proportion of excess mortality that was directly caused by SARS-CoV-2 infection and the changes in causes of death as an indirect consequence of the pandemic.
Funding: Bill & Melinda Gates Foundation, J Stanton, T Gillespie, and J and E Nordstrom.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests C Adolph reports support for the present manuscript from the Benificus Foundation for collection of data on state-level social distancing policies in the USA. X Dai reports support for the present manuscript from paid salary through employment at the Institute for Health Metrics and Evaluation and the University of Washington. N Fullman reports funding support from WHO as a consultant from June to September, 2019, and Gates Ventures since June, 2020, all outside the submitted work. S Nomura reports support for the present manuscript from a Ministry of Education, Culture, Sports, Science and Technology of Japan grant. D M Pigott reports support for the present manuscript from the Bill & Melinda Gates Foundation. D M Pigott also reports grants or contracts from the Bill & Melinda Gates Foundation, outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Death "With" COVID-19 and "Due to" COVID-19 from the medico-legal point of view.Med Sci Law. 2022 Oct;62(4):296. doi: 10.1177/00258024221099348. Epub 2022 May 6. Med Sci Law. 2022. PMID: 35521935 Free PMC article. No abstract available.
-
Conflicting COVID-19 excess mortality estimates.Lancet. 2023 Feb 11;401(10375):431-432. doi: 10.1016/S0140-6736(23)00116-2. Lancet. 2023. PMID: 36774147 Free PMC article. No abstract available.
-
Conflicting COVID-19 excess mortality estimates.Lancet. 2023 Feb 11;401(10375):431. doi: 10.1016/S0140-6736(23)00111-3. Lancet. 2023. PMID: 36774148 Free PMC article. No abstract available.
-
Conflicting COVID-19 excess mortality estimates.Lancet. 2023 Feb 11;401(10375):431. doi: 10.1016/S0140-6736(23)00112-5. Lancet. 2023. PMID: 36774149 Free PMC article. No abstract available.
-
Conflicting COVID-19 excess mortality estimates.Lancet. 2023 Feb 11;401(10375):432. doi: 10.1016/S0140-6736(23)00117-4. Lancet. 2023. PMID: 36774150 Free PMC article. No abstract available.
-
Conflicting COVID-19 excess mortality estimates.Lancet. 2023 Feb 11;401(10375):432-433. doi: 10.1016/S0140-6736(23)00115-0. Lancet. 2023. PMID: 36774151 Free PMC article. No abstract available.
References
-
- Li Y, Fang F, He M. Factors associated with nursing homes' late participation in COVID-19 reporting. J Am Geriatr Soc. 2020;68:2468–2469. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
