

Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN
- PMID: 35279527
- PMCID: PMC9161394
- DOI: 10.1016/j.esmoop.2022.100408
Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN
Abstract
Background: In the phase III CASPIAN study, first-line durvalumab in combination with etoposide plus either cisplatin or carboplatin (EP) significantly improved overall survival (OS) versus EP alone in extensive-stage small-cell lung cancer (ES-SCLC). Durvalumab plus tremelimumab plus EP numerically improved OS versus EP, but did not reach statistical significance. Here we report updated OS in censored patients after median follow-up of >3 years.
Patients and methods: 805 patients with treatment-naïve ES-SCLC were randomized 1 : 1 : 1 to durvalumab plus EP, durvalumab plus tremelimumab plus EP, or EP. The two primary endpoints were OS for durvalumab plus EP versus EP and for durvalumab plus tremelimumab plus EP versus EP.
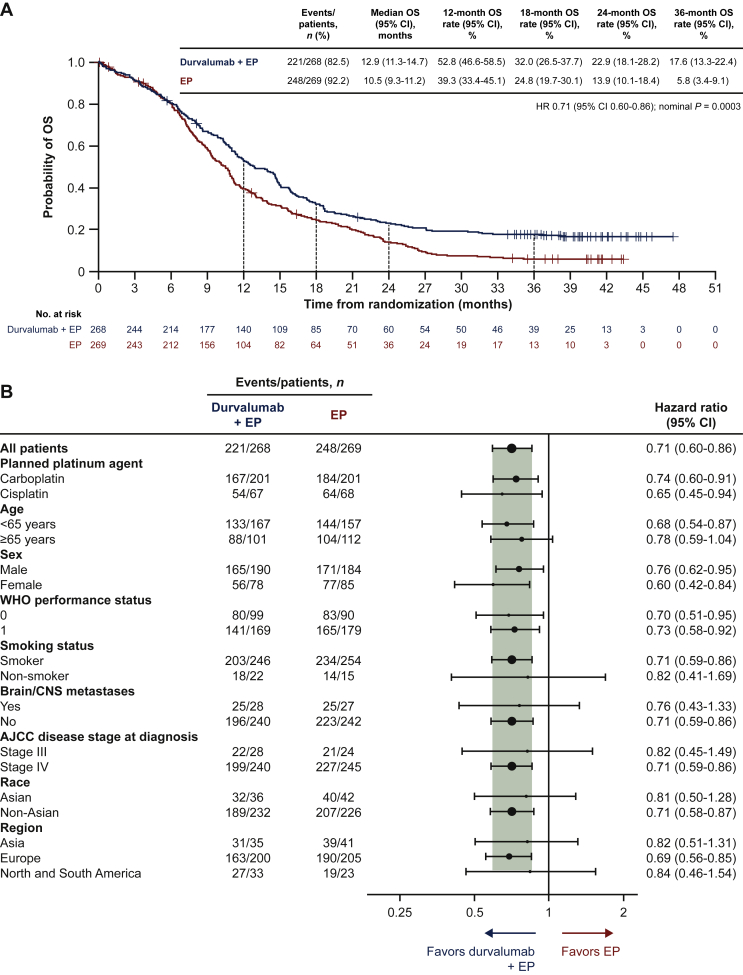
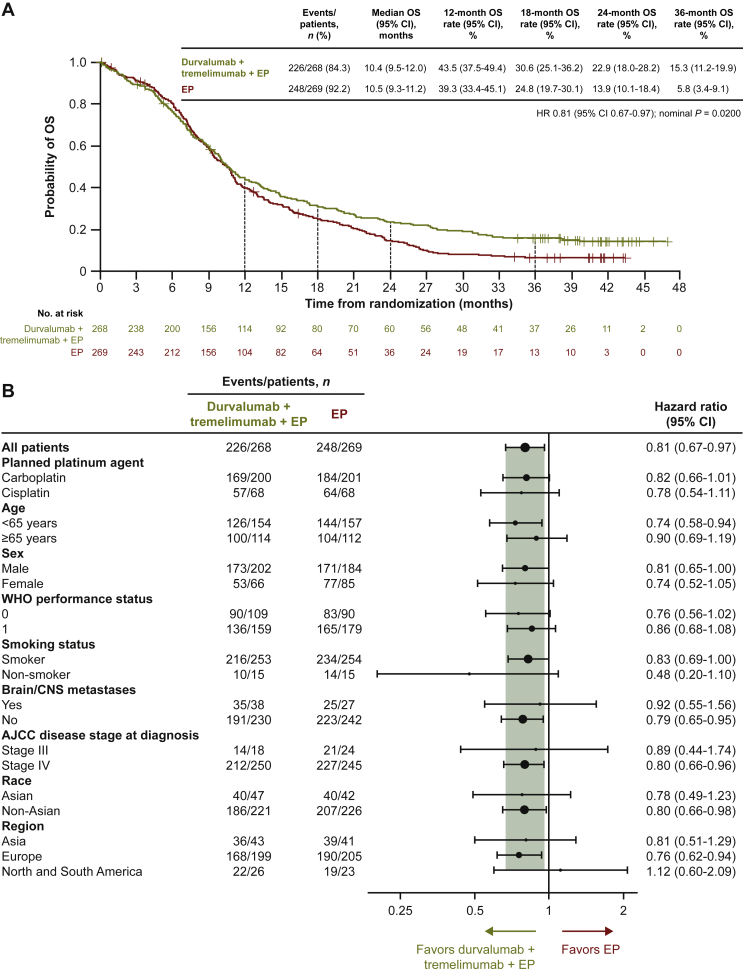
Results: As of 22 March 2021 (median follow-up 39.4 months, 86% maturity), durvalumab plus EP continued to demonstrate improved OS versus EP: hazard ratio (HR) 0.71 [95% confidence interval (CI) 0.60-0.86; nominal P = 0.0003]; median OS was 12.9 versus 10.5 months, and 36-month OS rate was 17.6% versus 5.8%. Durvalumab plus tremelimumab plus EP continued to numerically improve OS versus EP: HR 0.81 (95% CI: 0.67-0.97; nominal P = 0.0200); median OS was 10.4 months, and 36-month OS rate was 15.3%. Twenty-seven and nineteen patients in the durvalumab plus EP and durvalumab plus tremelimumab plus EP arms, respectively, remained on durvalumab treatment at data cut-off.
Conclusions: Three times more patients were estimated to be alive at 3 years when treated with durvalumab plus EP versus EP, with the majority still receiving durvalumab at data cut-off, further establishing durvalumab plus EP as first-line standard of care for ES-SCLC.
Keywords: CASPIAN; durvalumab; extensive-stage SCLC; overall survival; tremelimumab.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure LPA reports receiving grants from AstraZeneca, Bristol-Myers Squibb, MSD, and Pfizer; consulting fees from Amgen, AstraZeneca, Bayer, Blueprint Medicines, Bristol-Myers Squibb, Ipsen, Lilly, Merck, Mirati, MSD, Novartis, Pfizer, PharmaMar, Roche, Sanofi, and Servier; and honoraria from AstraZeneca, Janssen, Merck, Mirati, and Sanofi, and reports a leadership role with Genomica and Altum Sequencing, all outside the submitted work. YC reports receiving honoraria from Amgen, AstraZeneca, Bristol-Myers Squibb, Guardant Health, Jazz Pharmaceutical, Merck, Pfizer, and Takeda; and a research contract and support for meeting attendance/travel from Ipsen, all outside the submitted work. NR reports receiving honoraria from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Hoffmann-La Roche, Lilly, Merck, MSD, Pfizer, and Takeda; and consulting fees from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Hoffmann-La Roche, Merck, MSD, Pfizer, and Takeda, all outside the submitted work. KH reports receiving grants and personal fees from AstraZeneca during the conduct of the study; grants from Bristol-Myers Squibb, Chugai, Lilly, and MSD outside the submitted work; and honoraria from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Chugai, Lilly, MSD, Nippon Kayaku, Ono, Pfizer, Taiho, and Takeda outside the submitted work. MJH reports receiving speakers’ honoraria from AstraZeneca, Boehringer Ingelheim, MSD, Pfizer, Roche, and Takeda outside the submitted work. MCG reports receiving grants from AstraZeneca and Merck, and personal fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, GlaxoSmithKline, Merck, Novartis, Pfizer, Roche, and Takeda, all outside the submitted work. EM reports receiving grants from AstraZeneca during the conduct of the study and grants from Roche outside the submitted work. HM and TD report full-time employment and stock ownership with AstraZeneca. HJ reports full-time employment and stock ownership with AstraZeneca, and a patent pending for the CASPIAN study trial design. JWG reports receiving research grants from AbbVie, AstraZeneca, Bristol-Myers Squibb, Genentech, and Merck; consulting fees from AbbVie, AstraZeneca, Bristol-Myers Squibb, and Genentech; and support for travel from AstraZeneca all outside the submitted work. All other authors have declared no conflicts of interest. Data sharing Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data-sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Figures
References
-
- Paz-Ares L., Dvorkin M., Chen Y., et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929–1939. - PubMed
-
- Horn L., Mansfield A.S., Szczesna A., et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
