

Construction of a Non-Mutually Exclusive Decision Tree for Medication Recommendation of Chronic Heart Failure
- PMID: 35280259
- PMCID: PMC8904717
- DOI: 10.3389/fphar.2021.758573
Construction of a Non-Mutually Exclusive Decision Tree for Medication Recommendation of Chronic Heart Failure
Abstract
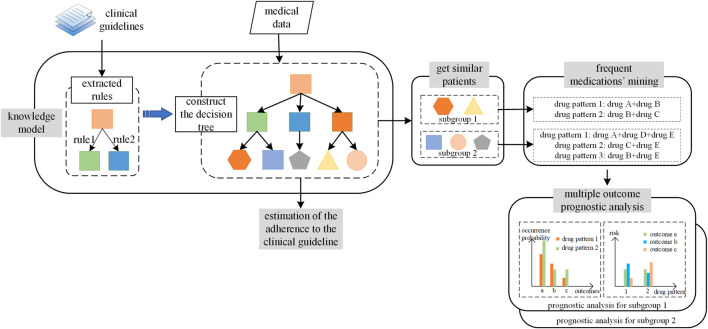
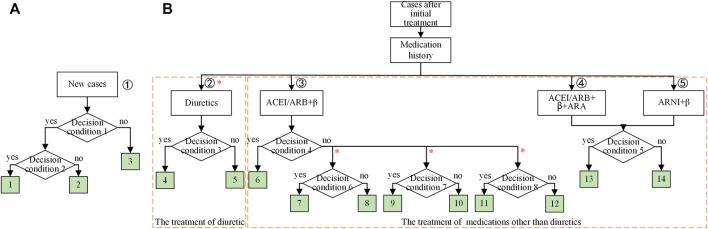
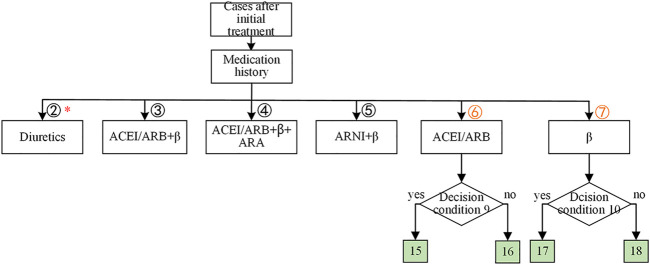
Objective: Although guidelines have recommended standardized drug treatment for heart failure (HF), there are still many challenges in making the correct clinical decisions due to the complicated clinical situations of HF patients. Each patient would satisfy several recommendations, meaning the decision tree of HF treatment should be nonmutually exclusive, and the same patient would be allocated to several leaf nodes in the decision tree. In the current study, we aim to propose a way to ensemble a nonmutually exclusive decision tree for recommendation system for complicated diseases, such as HF. Methods: The nonmutually exclusive decision tree was constructed via knowledge rules summarized from the HF clinical guidelines. Then similar patients were defined as those who followed the same pattern of leaf node allocation according to the decision tree. The frequent medication patterns for each similar patient were mined using the Apriori algorithms, and we also carried out the outcome prognosis analyses to show the capability for the evidence-based medication recommendations of our nonmutually exclusive decision tree. Results: Based on a large database that included 29,689 patients with 84,705 admissions, we tested the framework for HF treatment recommendation. In the constructed decision tree, the HF treatment recommendations were grouped into two independent parts. The first part was recommendations for new cases, and the second part was recommendations when patients had different historical medication. There are 14 leaf nodes in our decision tree, and most of the leaf nodes had a guideline adherence of around 90%. We reported the top 10 popular similar patients, which accounted for 32.84% of the whole population. In addition, the multiple outcome prognosis analyses were carried out to assess the medications for one of the subgroups of similar patients. Our results showed even for the subgroup of the same similar patients that no one medication pattern would benefit all outcomes. Conclusion: In the present study, the methodology to construct a nonmutually exclusive decision tree for medication recommendations for HF and its application in CDSS was proposed. Our framework is universal for most diseases and could be generally applied in developing the CDSS for treatment.
Keywords: chronic heart failure; clinical decision support system (CDSS); decision tree; machine learning; medication recommendation; treatment.
Copyright © 2022 Bai, Yao, Jiang, Bian, Zhou, Sun, Hu, Sun, Xie and He.
Conflict of interest statement
Authors HY, XJ, JZ, XS, GH, and GX were employed by the company Ping An Health Technology. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Agrawal R., Srikant R. (1994). Fast algorithms for mining association rules. Proc. 20th int. conf. very large data bases, VLDB 1215, 487–499.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous