

Neoadjuvant immunotherapy or chemoimmunotherapy in non-small cell lung cancer: a systematic review and meta-analysis
- PMID: 35280319
- PMCID: PMC8902081
- DOI: 10.21037/tlcr-22-75
Neoadjuvant immunotherapy or chemoimmunotherapy in non-small cell lung cancer: a systematic review and meta-analysis
Abstract
Background: In recent years, a series of clinical trials have explored the application of neoadjuvant immunotherapy or chemoimmunotherapy in non-small cell lung cancer (NSCLC). However, no randomized control trials comparing neoadjuvant immunotherapy with chemoimmunotherapy have yet been reported. This study aimed to summarize and compare the efficacy and safety of neoadjuvant immunotherapy and chemoimmunotherapy in NSCLC.
Methods: Literature focusing on the efficacy and safety of neoadjuvant immunotherapy or chemoimmunotherapy in NSCLC published before June 2021 was retrieved from PubMed, Embase, and the Cochrane Library. Study endpoints included major pathological response (MPR), complete pathological response (pCR), treatment-related adverse events (TRAEs), severe adverse events (SAEs), resection rate, surgical delay rate, and conversion to thoracotomy. The risk of bias was assessed using the Cochrane bias risk assessment tool. Subgroup and sensitivity analyses were further performed.
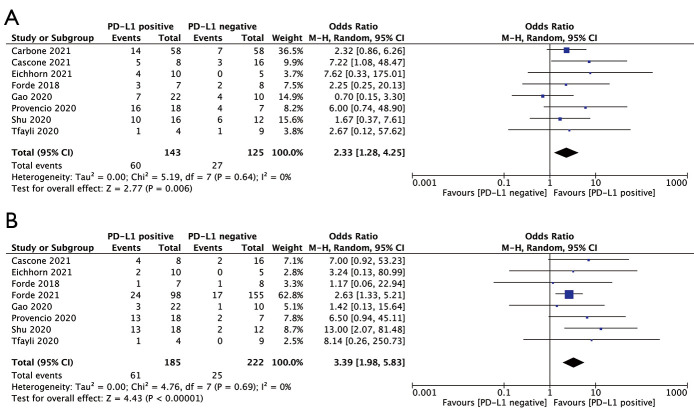
Results: A total of 988 patients from 16 studies were included in this meta-analysis. For patients who received neoadjuvant immunotherapy with single/combined ICIs or chemoimmunotherapy, the pooled MPR rate was 43.5% and the pooled pCR rate was 21.9%. The pooled incidence of TRAEs and SAEs were 54.8% and 15.3%, respectively. The pooled resection rate was 85.8%, the surgical delay rate was 7.4%, and the conversion rate was 17.4%. Patients who received neoadjuvant chemoimmunotherapy had remarkably improved pathological response (MPR rate: 53.3% vs. 28.6%; pCR rate: 28.6% vs. 9.9%) compared with those receiving neoadjuvant single-agent immunotherapy, while the incidence of SAEs (18.0% vs. 12.3%) and surgical delay rate (3.8% vs. 7.4%) did not significantly increase. Neoadjuvant nivolumab combined with ipilimumab also achieved a high pCR rate (28.6%) with tolerable toxicity. Nivolumab- and pembrolizumab-based neoadjuvant therapy showed a higher MPR rate (nivolumab 51.5%, pembrolizumab 46.8%) and pCR rate (nivolumab 29.1%, pembrolizumab 31.5%). Besides, patients with positive programmed death-ligand 1 (PD-L1) expression [tumor proportion score (TPS) ≥1%] exhibited favorable pathological responses than PD-L1 negative patients.
Discussion: Overall, neoadjuvant immunotherapy or chemoimmunotherapy is effective and safe in NSCLC. Compared with single-agent immunotherapy, neoadjuvant chemoimmunotherapy provides a significant improvement in pathological response without increasing the incidence of SAEs or surgical delay. These results need further confirmation by more large-scale randomized controlled trials.
Keywords: Non-small cell lung cancer (NSCLC); efficacy and safety; immune checkpoint inhibitors (ICIs); neoadjuvant chemoimmunotherapy; neoadjuvant immunotherapy.
2022 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-22-75/coif). Prof. SY serves as an unpaid editorial board member of Translational Lung Cancer Research from October 2021 to September 2023. The other authors have no conflicts of interest to declare.
Figures





References
LinkOut - more resources
Full Text Sources
Research Materials