

An Analysis of Computed Tomography Imaging Features and Predictive Factors for Postoperative Recurrence and Metastasis of Abdominal Paragangliomas
- PMID: 35280711
- PMCID: PMC8885278
- DOI: 10.1155/2022/8638588
An Analysis of Computed Tomography Imaging Features and Predictive Factors for Postoperative Recurrence and Metastasis of Abdominal Paragangliomas
Abstract
Methods: We studied 51 abdominal PGL patients at the First Affiliated Hospital of Bengbu Medical College, Tongde Hospital, and Sir Run Shaw Hospital, Hangzhou, Zhejiang Province, China, from June 2009 to May 2019. Thereafter, the clinical research data, tumor biomarkers, and CT features were compared between the aggressive PGLs and the nonaggressive PGLs using independent-samples t-tests and chi-square tests.
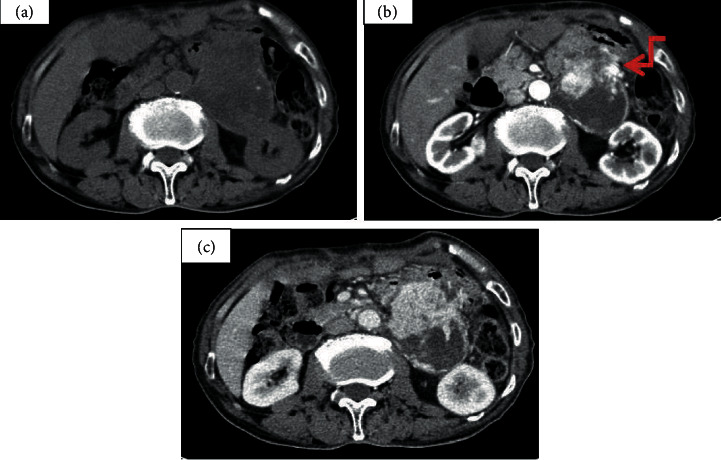
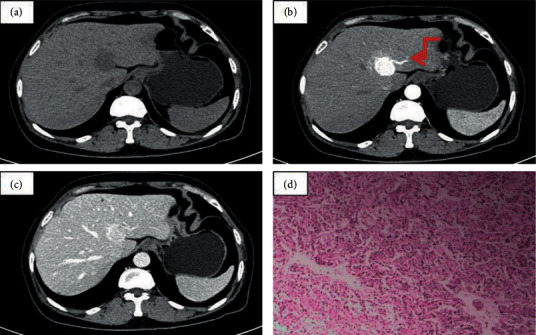
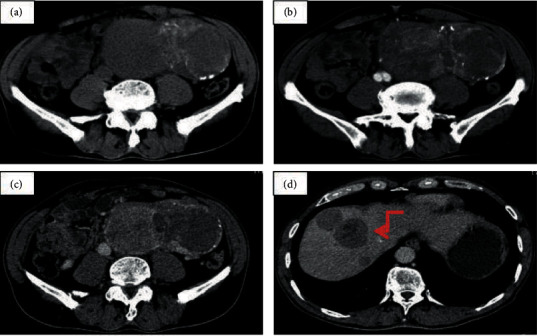
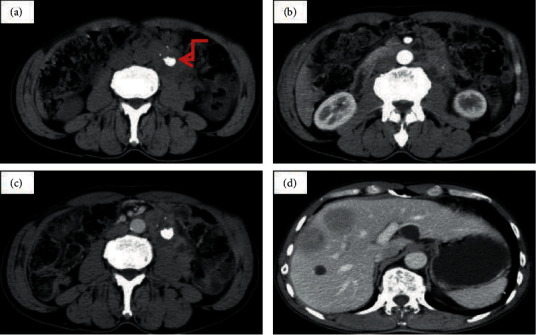
Results: Of the 51 cases, 43 were benign and 8 had malignant tendencies. Postoperative recurrence and metastasis were more likely to occur when the tumor diameter was >8 cm or/and the enhancement degree was not obvious. Clinical symptoms, tumor markers, sex, age, and CT image characteristics including morphology, presence of cystic degeneration, "pointed peach" sign, calcification, hemorrhage, enlarged lymph nodes, and peritumor and intratumor blood vessels were not significantly different between the two groups (p > 0.05).
Conclusion: Our findings suggest that CT features, including size >8 cm and enhancement degree, could provide important evidence to assess risk factors for aggressive PGLs.
Copyright © 2022 Bailing Dai et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest regarding the publication of this paper.
Figures
Similar articles
-
CT and MR Imaging Findings of Pancreatic Paragangliomas: A Case Report.Medicine (Baltimore). 2016 Mar;95(9):e2959. doi: 10.1097/MD.0000000000002959. Medicine (Baltimore). 2016. PMID: 26945413 Free PMC article.
-
A rare case of multiple paragangliomas in the head and neck, retroperitoneum and duodenum: A case report and review of the literature.Front Endocrinol (Lausanne). 2023 Jan 10;13:1054468. doi: 10.3389/fendo.2022.1054468. eCollection 2022. Front Endocrinol (Lausanne). 2023. PMID: 36704041 Free PMC article. Review.
-
[Analysis on CT in diagnosis of lymph node metastasis of thoracic esophageal cancer with minimum diameter greater than 1 cm].Zhonghua Wai Ke Za Zhi. 2019 Aug 1;57(8):601-606. doi: 10.3760/cma.j.issn.0529-5815.2019.08.008. Zhonghua Wai Ke Za Zhi. 2019. PMID: 31422630 Chinese.
-
GROWTH RATE OF PARAGANGLIOMAS RELATED TO GERMLINE MUTATIONS OF THE SDHX GENES.Endocr Pract. 2017 Mar;23(3):342-352. doi: 10.4158/EP161377.OR. Epub 2016 Dec 14. Endocr Pract. 2017. PMID: 27967220
-
Malignant extra-adrenal pancreatic paraganglioma: case report and literature review.BMC Cancer. 2013 Oct 20;13:486. doi: 10.1186/1471-2407-13-486. BMC Cancer. 2013. PMID: 24138700 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
