

The Clinical and Prognostic Impact of the Choice of Surgical Approach to Fourth Ventricular Tumors in a Single-Center, Single-Surgeon Cohort of 92 Consecutive Pediatric Patients
- PMID: 35280797
- PMCID: PMC8912940
- DOI: 10.3389/fonc.2022.821738
The Clinical and Prognostic Impact of the Choice of Surgical Approach to Fourth Ventricular Tumors in a Single-Center, Single-Surgeon Cohort of 92 Consecutive Pediatric Patients
Abstract
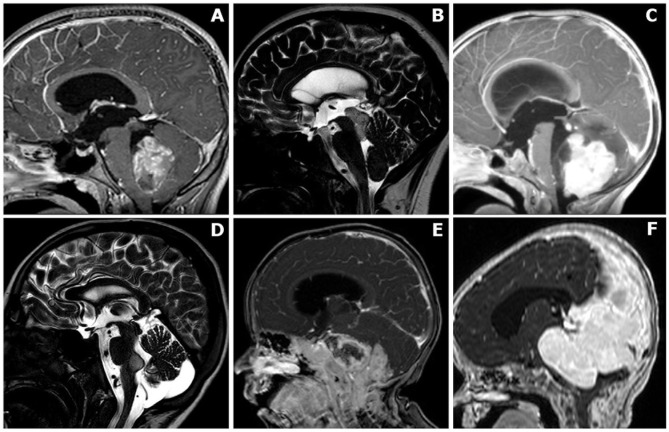
Objective: A single-institution cohort of 92 consecutive pediatric patients harboring tumors involving the fourth ventricle, surgically treated via the telovelar or transvermian approach, was retrospectively reviewed in order to analyze the impact of surgical route on surgery-related outcomes and cumulative survival.
Methods: Clinical, radiological, surgical, and pathology details were retrospectively analyzed. We selected n = 6 surgery-related clinical and radiological outcomes: transient and permanent neurological deficits, duration of assisted ventilation, postoperative new onset medical events, postoperative cerebellar mutism, and extent of resection. We built univariate and multivariate logistic models to analyze the significance of relationships between the surgical routes and the outcomes. Cumulative survival (CS) was estimated by the cohort approach.
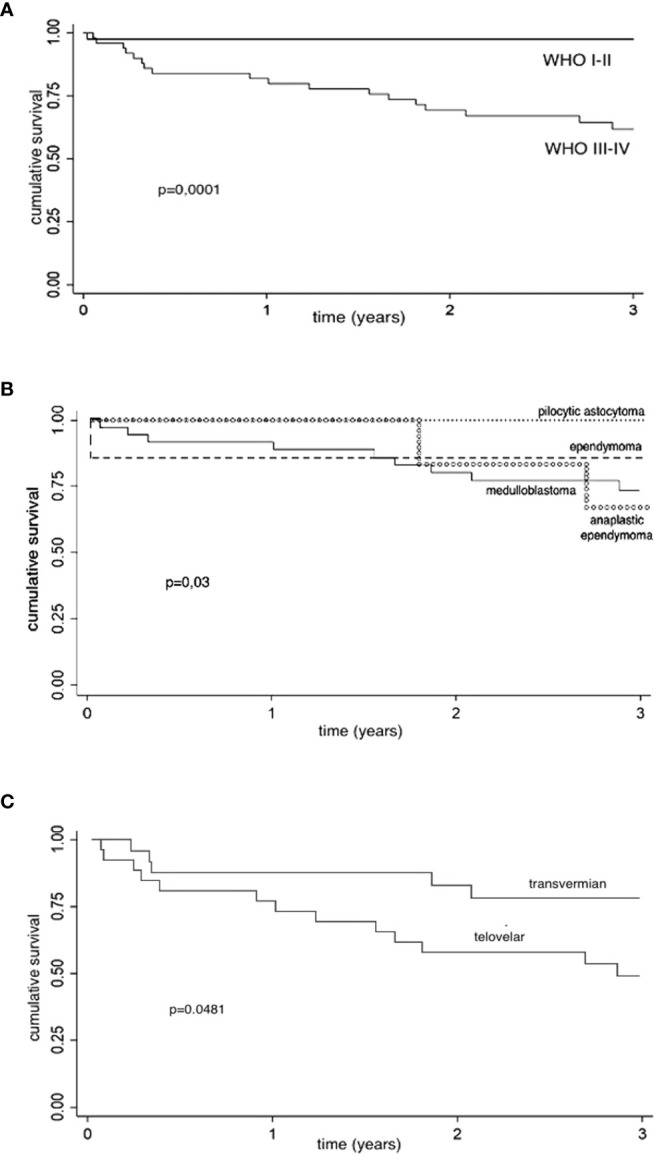
Results: There were 53 girls and 39 boys (mean age, 83 months). Telovelar approach was performed in 51 cases and transvermian approach in 41 cases. Early postoperative MRI studies showed complete removal in 57 cases (62%) and measurable residual tumor in 35 cases (38%). The average tumor residual volume was 1,316 cm3 (range, 0.016-4.231 cm3; median value, 0.9875 cm3). Residual disease was more often detected on immediate postop MRI after telovelar approach, but the difference was not significant. Cerebellar mutism was observed in 10 cases (11%). No significant difference in the onset of cerebellar mutism was detected between telovelar and transvermian approach. The choice of surgical approach did not significantly modify any other postoperative outcome and 1-/3-year CS of high-grade surgically treated tumors.
Conclusions: With the limitation of a single-center, single-surgeon retrospective series, our findings offer significant data to reconsider the real impact of the choice of the surgical route to the fourth ventricle on the incidence of cerebellar mutism and surgery-related morbidity. This seems to be in line with some recent reports in the literature. Surgical approach to the fourth ventricle should be individualized according to the location of the tumor, degree of vermian infiltration, and lateral and upward extension. Telovelar and transvermian approaches should not be considered alternative but complementary. Pediatric neurosurgeons should fully master both approaches and choose the one that they consider the best for the patient based on a thorough and careful evaluation of pre-operative imaging.
Keywords: cerebellar mutism; children; fourth ventricle; telovelar; transvermian.
Copyright © 2022 Onorini, Spennato, Orlando, Savoia, Calì, Russo, De Martino, de Santi, Mirone, Ruggiero, Quaglietta and Cinalli.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Predictors of postoperative complications and functional outcomes in pediatric patients with surgically treated fourth ventricle tumors.Acta Neurochir (Wien). 2023 Dec;165(12):4279-4292. doi: 10.1007/s00701-023-05729-w. Epub 2023 Aug 3. Acta Neurochir (Wien). 2023. PMID: 37535206
-
Telovelar surgical approach.Neurosurg Rev. 2021 Feb;44(1):61-76. doi: 10.1007/s10143-019-01190-5. Epub 2019 Dec 5. Neurosurg Rev. 2021. PMID: 31807931 Review.
-
The surgical treatment of tumors of the fourth ventricle: a single-institution experience.J Neurosurg. 2018 Feb;128(2):339-351. doi: 10.3171/2016.11.JNS161167. Epub 2017 Apr 14. J Neurosurg. 2018. PMID: 28409732
-
Fourth ventricle tumors in children: complications and influence of surgical approach.J Neurosurg Pediatr. 2020 Oct 23;27(1):52-61. doi: 10.3171/2020.6.PEDS2089. Print 2021 Jan 1. J Neurosurg Pediatr. 2020. PMID: 33096529
-
Telovelar Approach to Fourth Ventricle Tumors: Highlights and Limitations.World Neurosurg. 2015 Jun;83(6):1141-7. doi: 10.1016/j.wneu.2015.01.039. Epub 2015 Feb 16. World Neurosurg. 2015. PMID: 25698525 Review.
Cited by
-
A predictive model for cerebellar mutism syndrome based on lesion map in children with medulloblastoma.Eur Radiol. 2025 Jun;35(6):3294-3304. doi: 10.1007/s00330-024-11264-8. Epub 2024 Dec 10. Eur Radiol. 2025. PMID: 39658685
-
Predictors of postoperative complications and functional outcomes in pediatric patients with surgically treated fourth ventricle tumors.Acta Neurochir (Wien). 2023 Dec;165(12):4279-4292. doi: 10.1007/s00701-023-05729-w. Epub 2023 Aug 3. Acta Neurochir (Wien). 2023. PMID: 37535206
-
Adult Medulloblastoma: Updates on Current Management and Future Perspectives.Cancers (Basel). 2022 Jul 29;14(15):3708. doi: 10.3390/cancers14153708. Cancers (Basel). 2022. PMID: 35954372 Free PMC article. Review.
-
Telovelar versus transvermian approach to tumors of the fourth ventricle and their impact on postoperative neurological complications: A multicenter study.Surg Neurol Int. 2023 Apr 7;14:124. doi: 10.25259/SNI_167_2023. eCollection 2023. Surg Neurol Int. 2023. PMID: 37151430 Free PMC article.
-
Pilocytic astrocytoma: The paradigmatic entity in low‑grade gliomas (Review).Oncol Lett. 2024 Feb 8;27(4):146. doi: 10.3892/ol.2024.14279. eCollection 2024 Apr. Oncol Lett. 2024. PMID: 38385109 Free PMC article. Review.
References
-
- Frazier CH. Remarks Upon the Surgical Aspects of Tumors of the Cerebellum. NY State J Med (1905) 18:272–280, 332–337.
-
- Craig WM, Kernohan JW. Tumors of the Fourth Ventricle. JAMA (1938) 111(26):2370–7. doi: 10.1001/jama.1938.02790520026006 - DOI
-
- Dandy WE. Surgery of the Brain. In: Lewis D, editor. Practice of Surgery. Vol 12. Hagerstown, Md: WF Prior; (1932). p. 625–31.
-
- Özek MM, Cinalli G, Maixner W, Sainte-Rose C. Posterior Fossa Tumors in Children. Switzerland: Springer International Publishing; (2015), 948. doi: 10.1007/978-3-319-11274-9 - DOI
-
- Matsushima T. Microsurgical Anatomy of the Cerebellomedullary Fissure and Variations of the Transcerebellomedullary Fissure Approach. In: Matsushima T, editor. Microsurgical Anatomy and Surgery of the Posterior Cranial Fossa. Tokyo: Springer; (2015). p. 73–99. doi: 10.1007/978-4-431-54183-7_7 - DOI
LinkOut - more resources
Full Text Sources