

Robotic Versus Laparoscopic Pancreaticoduodenectomy: An Up-To-Date System Review and Meta-Analysis
- PMID: 35280811
- PMCID: PMC8914533
- DOI: 10.3389/fonc.2022.834382
Robotic Versus Laparoscopic Pancreaticoduodenectomy: An Up-To-Date System Review and Meta-Analysis
Abstract
Background: Although minimally invasive pancreaticoduodenectomy has gained worldwide interest, there are limited comparative studies between two minimally invasive pancreaticoduodenectomy techniques. This meta-analysis aimed to compare the safety and efficacy of robotic and laparoscopic pancreaticoduodenectomy (LPD), especially the difference in the perioperative and short-term oncological outcomes.
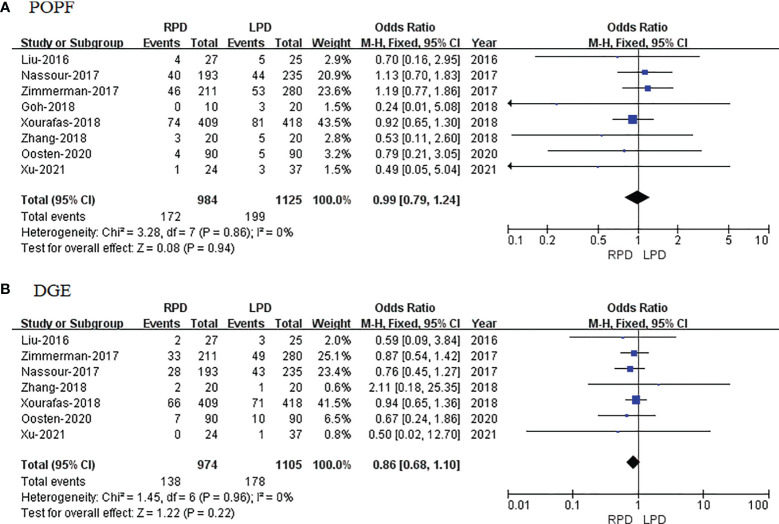
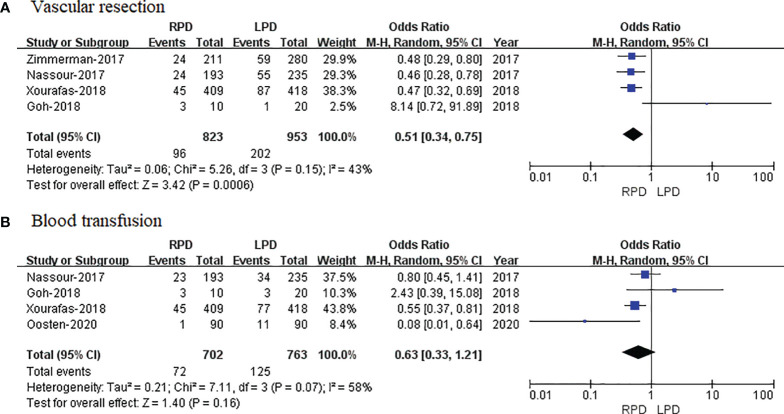
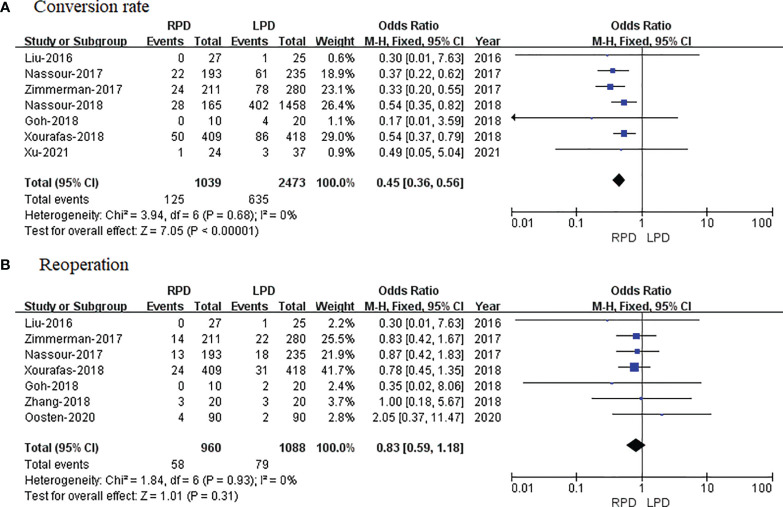
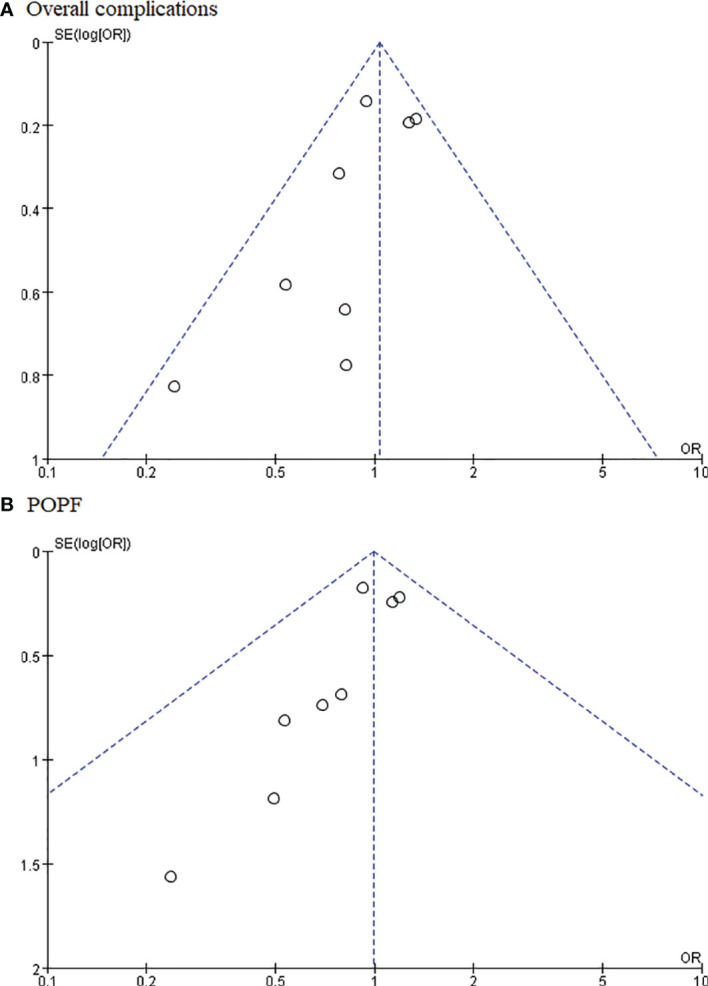
Methods: PubMed, China National Knowledge Infrastructure (CNKI), Wanfang Data, Web of Science, and EMBASE were searched based on a defined search strategy to identify eligible studies before July 2021. Data on operative times, blood loss, overall morbidity, major complications, vascular resection, blood transfusion, postoperative pancreatic fistula (POPF), delayed gastric emptying (DGE), conversion rate, reoperation, length of hospital stay (LOS), and lymph node dissection were subjected to meta-analysis.
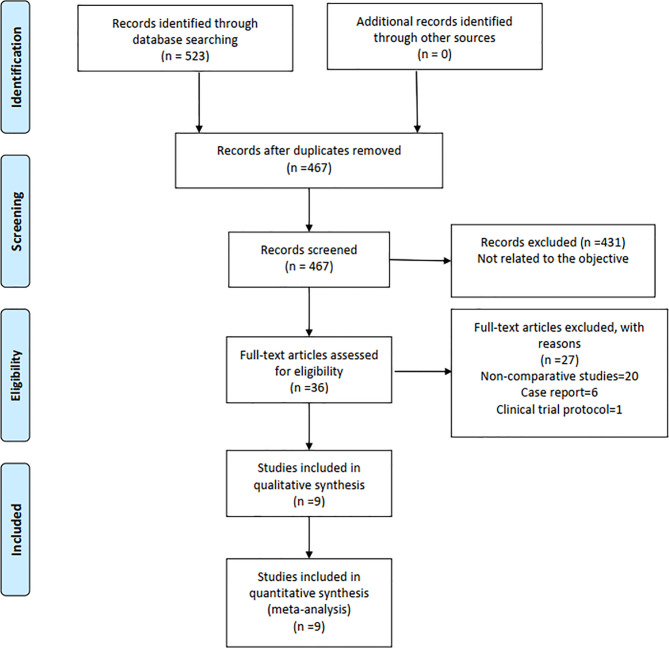
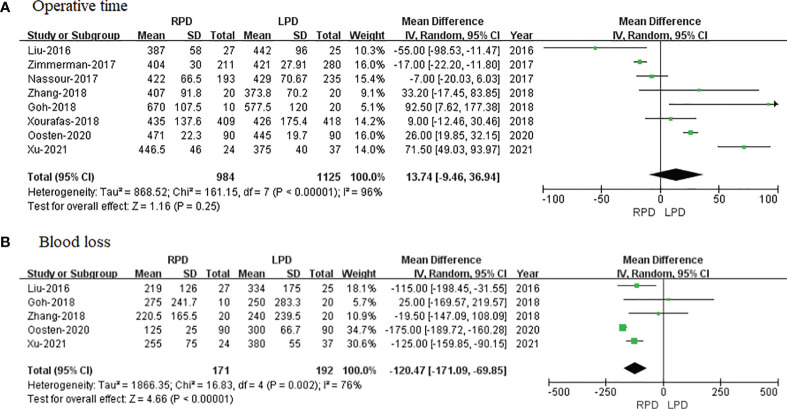
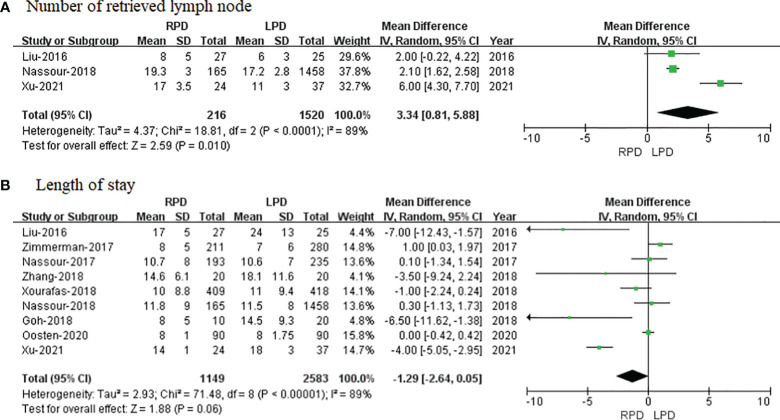
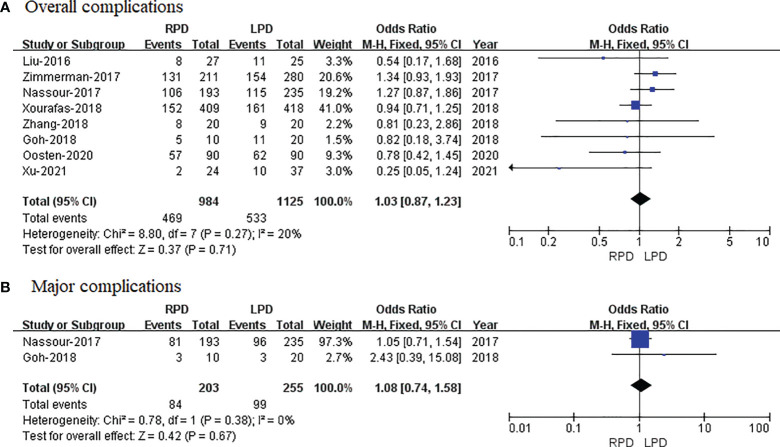
Results: Overall, the final analysis included 9 retrospective studies comprising 3,732 patients; 1,149 (30.79%) underwent robotic pancreaticoduodenectomy (RPD), and 2,583 (69.21%) underwent LPD. The present meta-analysis revealed nonsignificant differences in operative times, overall morbidity, major complications, blood transfusion, POPF, DGE, reoperation, and LOS. Alternatively, compared with LPD, RPD was associated with less blood loss (p = 0.002), less conversion rate (p < 0.00001), less vascular resection (p = 0.0006), and more retrieved lymph nodes (p = 0.01).
Conclusion: RPD is at least equivalent to LPD with respect to the incidence of complication, incidence and severity of DGE, and reoperation and length of hospital stay. Compared with LPD, RPD seems to be associated with less blood loss, lower conversion rate, less vascular resection, and more retrieved lymph nodes.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/#recordDetails, identifier CRD2021274057.
Keywords: Da Vinci; laparoscopic pancreaticoduodenectomy; meta-analysis; minimally invasive surgery; robotic pancreaticoduodenectomy.
Copyright © 2022 Ouyang, Zhang, Feng, Zhang, Ma and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources