

A Nomogram-Based Model to Predict Respiratory Dysfunction at 6 Months in Non-Critical COVID-19 Survivors
- PMID: 35280880
- PMCID: PMC8904385
- DOI: 10.3389/fmed.2022.781410
A Nomogram-Based Model to Predict Respiratory Dysfunction at 6 Months in Non-Critical COVID-19 Survivors
Abstract
Objective: To assess the prevalence of respiratory sequelae of Coronavirus disease 2019 (COVID-19) survivors at 6 months after hospital discharge and develop a model to identify at-risk patients.
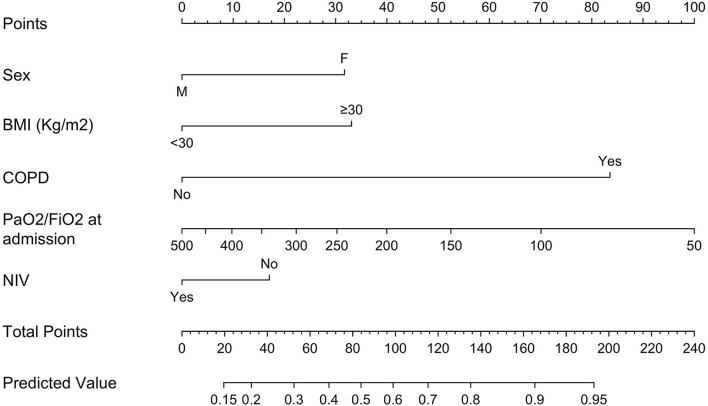
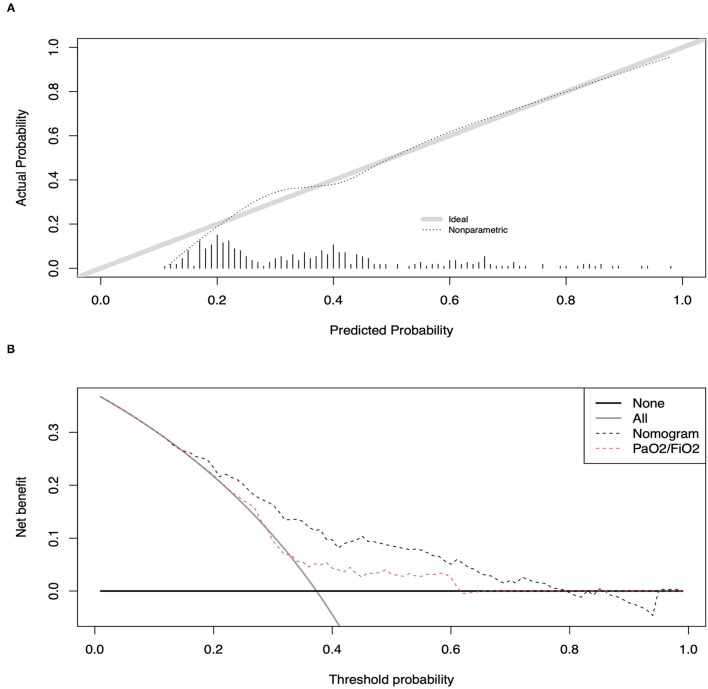
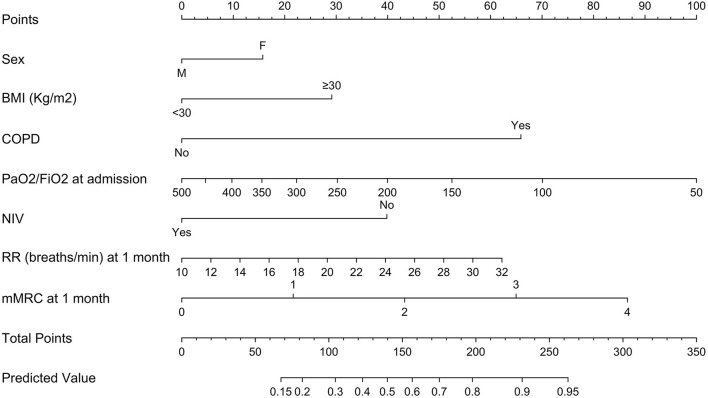
Patients and methods: In this prospective cohort study, hospitalized, non-critical COVID-19 patients evaluated at 6-month follow-up between 26 August, 2020 and 16 December, 2020 were included. Primary outcome was respiratory dysfunction at 6 months, defined as at least one among tachypnea at rest, percent predicted 6-min walking distance at 6-min walking test (6MWT) ≤ 70%, pre-post 6MWT difference in Borg score ≥ 1 or a difference between pre- and post-6MWT oxygen saturation ≥ 5%. A nomogram-based multivariable logistic regression model was built to predict primary outcome. Validation relied on 2000-resample bootstrap. The model was compared to one based uniquely on degree of hypoxemia at admission.
Results: Overall, 316 patients were included, of whom 118 (37.3%) showed respiratory dysfunction at 6 months. The nomogram relied on sex, obesity, chronic obstructive pulmonary disease, degree of hypoxemia at admission, and non-invasive ventilation. It was 73.0% (95% confidence interval 67.3-78.4%) accurate in predicting primary outcome and exhibited minimal departure from ideal prediction. Compared to the model including only hypoxemia at admission, the nomogram showed higher accuracy (73.0 vs 59.1%, P < 0.001) and greater net-benefit in decision curve analyses. When the model included also respiratory data at 1 month, it yielded better accuracy (78.2 vs. 73.2%) and more favorable net-benefit than the original model.
Conclusion: The newly developed nomograms accurately identify patients at risk of persistent respiratory dysfunction and may help inform clinical priorities.
Keywords: COVID-19; follow-up; long-term; prediction algorithm; respiratory sequelae.
Copyright © 2022 De Lorenzo, Magnaghi, Cinel, Vitali, Martinenghi, Mazza, Nocera, Cilla, Damanti, Compagnone, Ferrante, Conte, Benedetti, Ciceri and Rovere-Querini.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources