

Effect Evaluation of Platelet-Rich Plasma Combined with Vacuum Sealing Drainage on Serum Inflammatory Factors in Patients with Pressure Ulcer by Intelligent Algorithm-Based CT Image
- PMID: 35281950
- PMCID: PMC8906978
- DOI: 10.1155/2022/8916076
Effect Evaluation of Platelet-Rich Plasma Combined with Vacuum Sealing Drainage on Serum Inflammatory Factors in Patients with Pressure Ulcer by Intelligent Algorithm-Based CT Image
Retraction in
-
Retracted: Effect Evaluation of Platelet-Rich Plasma Combined with Vacuum Sealing Drainage on Serum Inflammatory Factors in Patients with Pressure Ulcer by Intelligent Algorithm-Based CT Image.Comput Math Methods Med. 2023 Dec 13;2023:9845010. doi: 10.1155/2023/9845010. eCollection 2023. Comput Math Methods Med. 2023. PMID: 38124913 Free PMC article.
Abstract
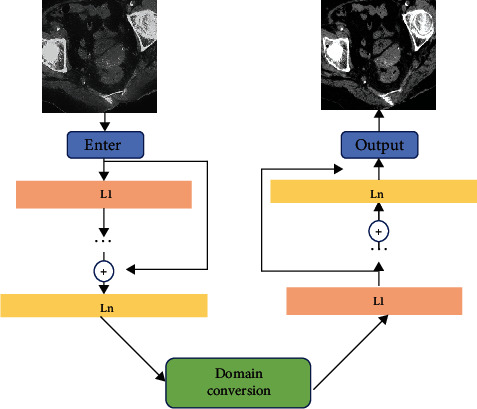
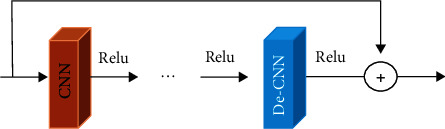
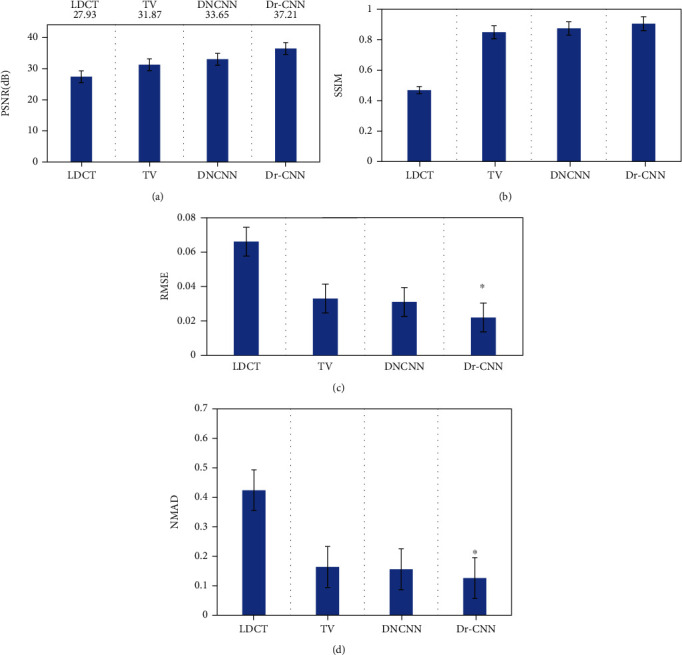
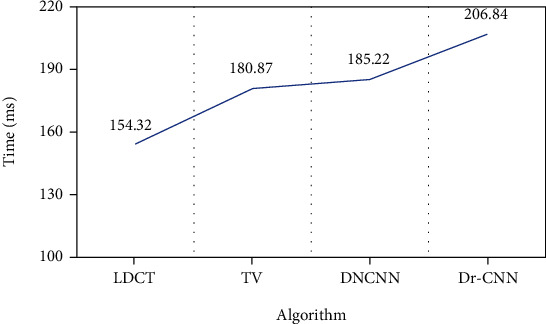
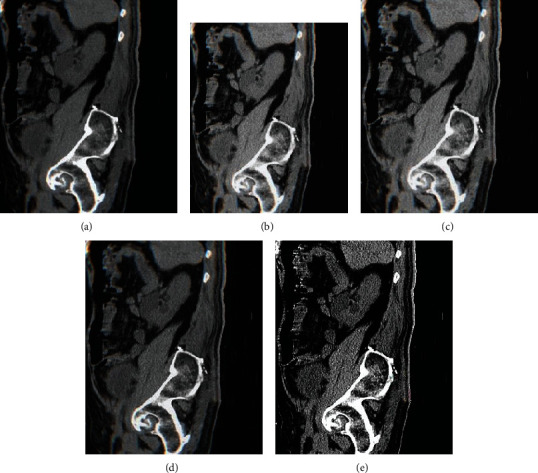
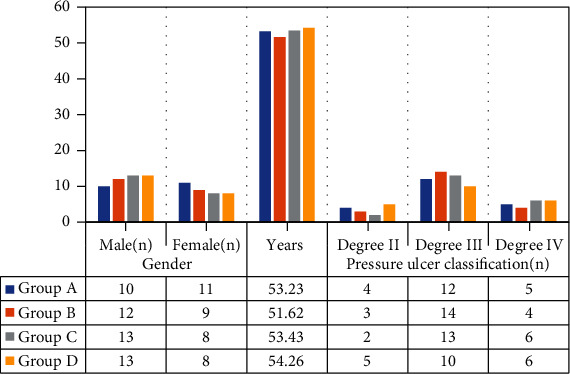
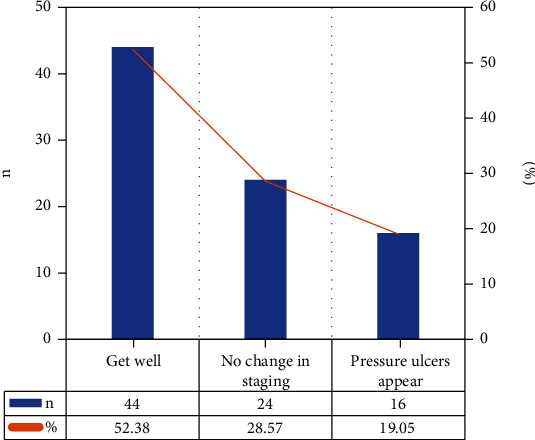
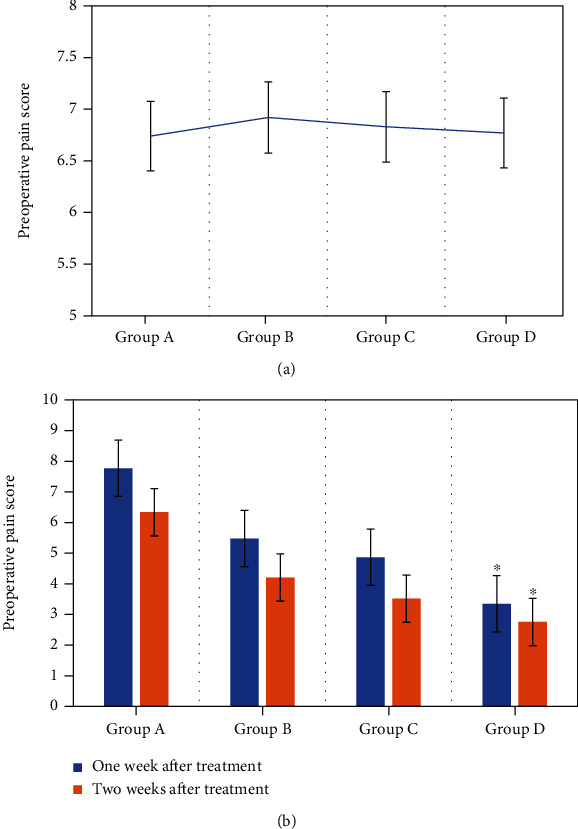
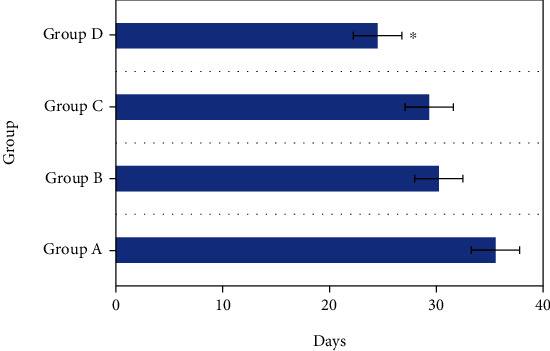
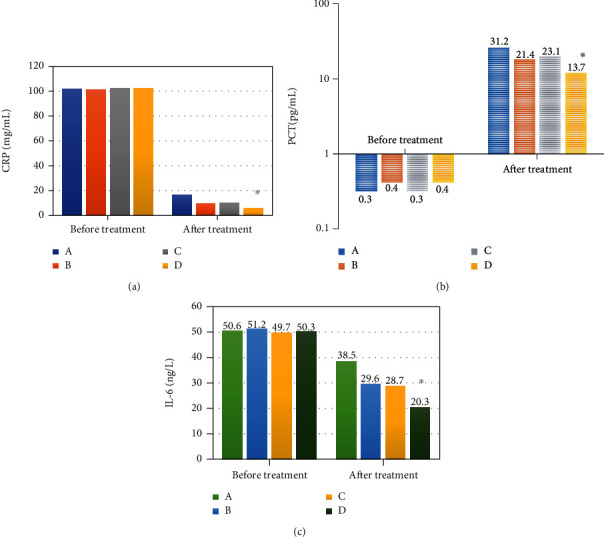
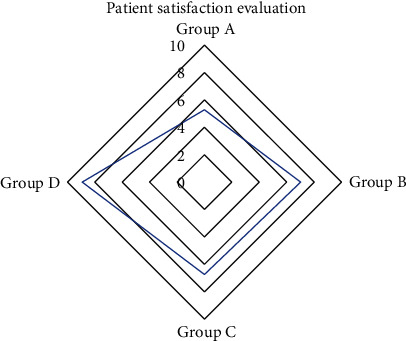
This work was to explore the efficacy of intelligent algorithm-based computed tomography (CT) to evaluate platelet-rich plasma (PRP) combined with vacuum sealing drainage (VSD) in the treatment of patients with pressure ulcers. Based on the u-net network structure, an image denoising algorithm based on double residual convolution neural network (Dr-CNN) was proposed to denoise the CT images. A total of 84 patients who were hospitalized in hospital were randomly divided into group A (without any intervention), group B (PRP treatment), group C (VSD treatment), and group D (PRP+VSD treatment). Procalcitonin (PCT) was detected by enzyme-linked immunosorbent assay (ELISA) combined with immunofluorescence method, C-reactive protein (CRP) was detected by rate reflectance turbidimetry (RRT), and interleukin-6 (IL-6) was detected by electrochemiluminescence method. The results showed that after treatment, 44 cases (52.38%) of pressure ulcers patients recovered, 24 cases (28.57%) had no change in stage, and 16 cases (19.04%) developed pressure ulcers. The pain scores of group D at 1 week (3.35 ± 0.56 points) and 2 weeks (2.76 ± 0.55 points) after treatment were significantly lower than those in group C (7.77 ± 0.58 points and 6.34 ± 0.44 points, respectively). The time of complete wound healing in group D (24.5 ± 2.32) was obviously lower in contrast to that in groups A, B, and C (35.54 ± 3.22 days, 30.23 ± 2 days, and 29.34 ± 2.15 days, respectively). In addition, the medical satisfaction of group D (8.74 ± 0.69) was significantly higher than that of groups A, B, and C (4.69 ± 0.85, 5.22 ± 0.31, and 5.18 ± 0.59, respectively). The levels of IL-6 and PCT in group D were lower than those in groups A, B, and C, and the differences were statistically significant (P < 0.01). The average values of peak signal to noise ratio (PSNR) and structural similarity index measure (SSIM) of the Dr-CNN network model were 37.21 ± 1.09 dB and 0.925 ± 0.01, respectively, which were higher than other algorithms. The mean values of root mean square error (MSE) and normalized mean absolute distance (NMAD) of the Dr-CNN network model were 0.022 ± 0.002 and 0.126 ± 0.012, respectively, which were significantly lower than other algorithms (P < 0.05). The experimental results showed that PrP combined with VSD could significantly reduce the inflammatory response of patients with pressure ulcers. PRP combined with VSD could significantly reduce the pain of dressing change for patients. Moreover, the performance model of image denoising algorithm based on double residual convolutional neural network was better than other algorithms.
Copyright © 2022 Jingzhe Yang et al.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Collier M. Pressure ulcer prevention: fundamentals for best practice. Acta Medica Croatica . 2016;70(Suppl 1):3–10. PMID: 29087640. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
