

Optimal and actual rates of Stereotactic Ablative Body Radiotherapy (SABR) utilisation for primary lung cancer in Australia
- PMID: 35282142
- PMCID: PMC8907547
- DOI: 10.1016/j.ctro.2022.03.001
Optimal and actual rates of Stereotactic Ablative Body Radiotherapy (SABR) utilisation for primary lung cancer in Australia
Abstract
Background and purpose: Radiotherapy utilisation rates considerably vary across different countries and service providers, highlighting the need to establish reliable benchmarks against which utilisation rates can be assessed. Here, optimal utilisation rates of Stereotactic Ablative Body Radiotherapy (SABR) for lung cancer are estimated and compared against actual utilisation rates to identify potential shortfalls in service provision.
Materials and methods: An evidence-based optimal utilisation model was constructed after reviewing practice guidelines and identifying indications for lung SABR based on the best available evidence. The proportions of patients likely to develop each indication were obtained, whenever possible, from Australian population-based studies. Sensitivity analysis was performed to account for variations in epidemiological data. Practice pattern studies were reviewed to obtain actual utilisation rates.
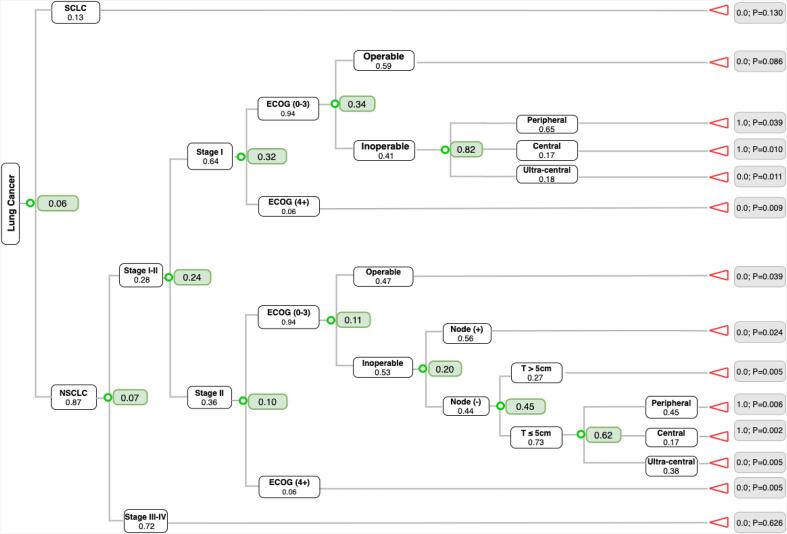
Results: A total of 6% of all lung cancer patients were estimated to optimally require SABR at least once during the course of their illness (95% CI: 4-6%). Optimal utilisation rates were estimated to be 32% for stage I and 10% for stage II NSCLC. Actual utilisation rates for stage I NSCLC varied between 6 and 20%. For patients with inoperable stage I, 27-74% received SABR compared to the estimated optimal rate of 82%.
Conclusion: The estimated optimal SABR utilisation rates for lung cancer can serve as useful benchmarks to highlight gaps in service delivery and help plan for more adequate and efficient provision of care. The model can be easily modified to determine optimal utilisation rates in other populations or updated to reflect any changes in practice guidelines or epidemiological data.
Keywords: Lung SABR; Optimal utilisation; Practice patterns; Utilisation gaps.
© 2022 Published by Elsevier B.V. on behalf of European Society for Radiotherapy and Oncology.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): a phase 3, open-label, randomised controlled trial.Lancet Oncol. 2019 Apr;20(4):494-503. doi: 10.1016/S1470-2045(18)30896-9. Epub 2019 Feb 12. Lancet Oncol. 2019. PMID: 30770291 Clinical Trial.
-
Stereotactic Ablative Body Radiotherapy Versus Radical Radiotherapy: Comparing Real-World Outcomes in Stage I Lung Cancer.Clin Oncol (R Coll Radiol). 2019 Oct;31(10):681-687. doi: 10.1016/j.clon.2019.07.013. Epub 2019 Jul 31. Clin Oncol (R Coll Radiol). 2019. PMID: 31377081
-
Estimation of an optimal chemotherapy utilisation rate for lung cancer: an evidence-based benchmark for cancer care.Lung Cancer. 2010 Sep;69(3):307-14. doi: 10.1016/j.lungcan.2009.11.017. Epub 2010 Jan 18. Lung Cancer. 2010. PMID: 20080315
-
Is radiofrequency ablation more effective than stereotactic ablative radiotherapy in patients with early stage medically inoperable non-small cell lung cancer?Interact Cardiovasc Thorac Surg. 2012 Aug;15(2):258-65. doi: 10.1093/icvts/ivs179. Epub 2012 May 10. Interact Cardiovasc Thorac Surg. 2012. PMID: 22581864 Free PMC article. Review.
-
Systematic review of economic evaluations on stereotactic ablative radiotherapy (SABR) compared to other radiotherapy techniques or surgical procedures for early-stage non-small cell lung cancer.Cost Eff Resour Alloc. 2023 Jan 16;21(1):4. doi: 10.1186/s12962-023-00415-1. Cost Eff Resour Alloc. 2023. PMID: 36647118 Free PMC article. Review.
Cited by
-
Utilisation of radiotherapy in lung cancer: A scoping narrative literature review with a focus on the introduction of evidence-based therapeutic approaches in Europe.Clin Transl Radiat Oncol. 2023 Dec 18;45:100717. doi: 10.1016/j.ctro.2023.100717. eCollection 2024 Mar. Clin Transl Radiat Oncol. 2023. PMID: 38226026 Free PMC article.
References
-
- Ettinger D.S., et al. Non-Small Cell Lung Cancer, Version 5.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2017;15:504–535. - PubMed
-
- Schneider B.J., et al. Stereotactic Body Radiotherapy for Early-Stage Non–Small-Cell Lung Cancer: American Society of Clinical Oncology Endorsement of the American Society for Radiation Oncology Evidence-Based Guideline. J Clin Oncol. 2017;36:710–719. - PubMed
-
- Delaney G., Barton M., Jacob S., Jalaludin B. A model for decision making for the use of radiotherapy in lung cancer. Lancet Oncol. 2003;4:120–128. - PubMed
-
- Vinod S.K., et al. Underutilization of radiotherapy for lung cancer in New South Wales. Australia Cancer. 2010;116:686–694. - PubMed
-
- Li W.W.L., et al. The influence of provider characteristics on resection rates and survival in patients with localized non-small cell lung cancer. Lung Cancer. 2008;60:441–451. - PubMed
LinkOut - more resources
Full Text Sources
