

Post-transplant Lymphoproliferative Disorder Following Cardiac Transplantation
- PMID: 35282339
- PMCID: PMC8904724
- DOI: 10.3389/fcvm.2022.787975
Post-transplant Lymphoproliferative Disorder Following Cardiac Transplantation
Abstract
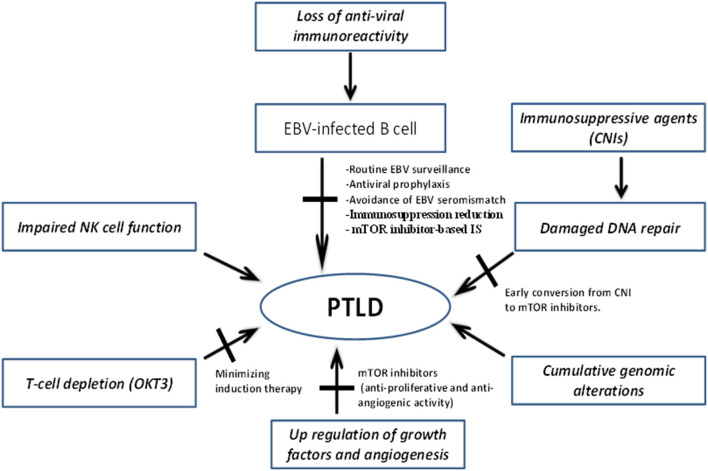
Post-transplant lymphoproliferative disorder (PTLD) is a spectrum of lymphoid conditions frequently associated with the Epstein Barr Virus (EBV) and the use of potent immunosuppressive drugs after solid organ transplantation. PTLD remains a major cause of long-term morbidity and mortality following heart transplantation (HT). Epstein-Barr virus (EBV) is a key pathogenic driver in many PTLD cases. In the majority of PTLD cases, the proliferating immune cell is the B-cell, and the impaired T-cell immune surveillance against infected B cells in immunosuppressed transplant patients plays a key role in the pathogenesis of EBV-positive PTLD. Preventive screening strategies have been attempted for PTLD including limiting patient exposure to aggressive immunosuppressive regimens by tailoring or minimizing immunosuppression while preserving graft function, anti-viral prophylaxis, routine EBV monitoring, and avoidance of EBV seromismatch. Our group has also demonstrated that conversion from calcineurin inhibitor to the mammalian target of rapamycin (mTOR) inhibitor, sirolimus, as a primary immunosuppression was associated with a decreased risk of PTLD following HT. The main therapeutic measures consist of immunosuppression reduction, treatment with rituximab and use of immunochemotherapy regimens. The purpose of this article is to review the potential mechanisms underlying PTLD pathogenesis, discuss recent advances, and review potential therapeutic targets to decrease the burden of PTLD after HT.
Keywords: Epstein-Barr virus; PTLD; heart transplantation; immunosuppression; mTOR inhibitors; rituximab.
Copyright © 2022 Asleh, Alnsasra, Habermann, Briasoulis and Kushwaha.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Buell JF, Gross TG, Woodle ES. Malignancy after transplantation. Transplantation. (2005) 80:S254–64. 10.1097/01.tp.0000186382.81130.ba - DOI - PubMed
-
- Penn I. Incidence and treatment of neoplasia after transplantation. J Heart Lung Transpl. (1993) 12:S328–36. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous