

Non-invasive Multimodality Imaging of Coronary Vulnerable Patient
- PMID: 35282382
- PMCID: PMC8907666
- DOI: 10.3389/fcvm.2022.836473
Non-invasive Multimodality Imaging of Coronary Vulnerable Patient
Abstract
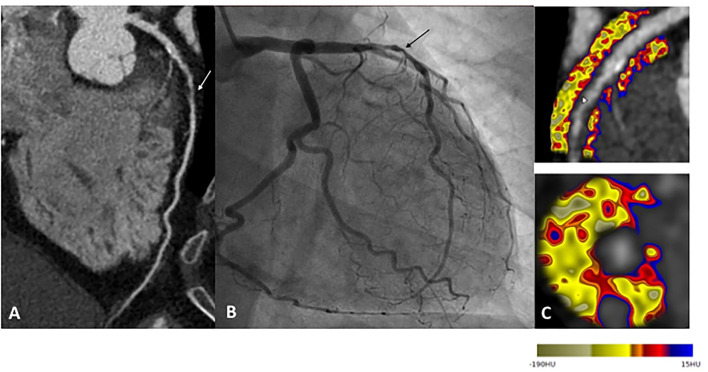
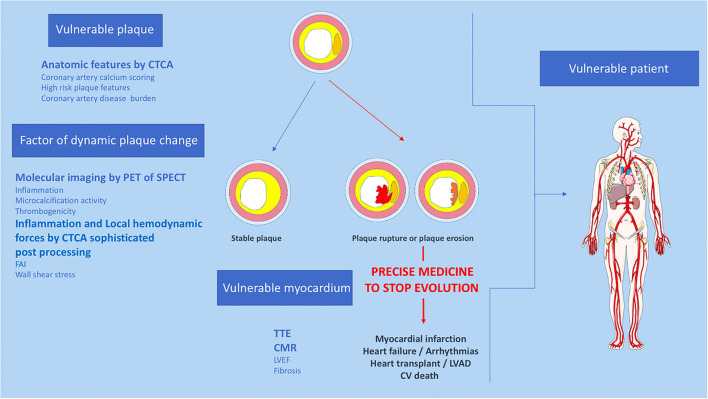
Atherosclerotic plaque rupture or erosion remain the primary mechanism responsible for myocardial infarction and the major challenge of cardiovascular researchers is to develop non-invasive methods of accurate risk prediction to identify vulnerable plaques before the event occurs. Multimodal imaging, by CT-TEP or CT-SPECT, provides both morphological and activity information about the plaque and cumulates the advantages of anatomic and molecular imaging to identify vulnerability features among coronary plaques. However, the rate of acute coronary syndromes remains low and the mechanisms leading to adverse events are clearly more complex than initially assumed. Indeed, recent studies suggest that the detection of a state of vulnerability in a patient is more important than the detection of individual sites of vulnerability as a target of focal treatment. Despite this evolution of concepts, multimodal imaging offers a strong potential to assess patient's vulnerability. Here we review the current state of multimodal imaging to identify vulnerable patients, and then focus on emerging imaging techniques and precision medicine.
Keywords: chronic coronary syndrome; coronary artery disease; multimodal imaging; risk stratification; vulnerable patient; vulnerable plaque.
Copyright © 2022 Canu, Broisat, Riou, Vanzetto, Fagret, Ghezzi, Djaileb and Barone-Rochette.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources