

Conventional fluoroscopy-guided versus zero-fluoroscopy catheter ablation of supraventricular tachycardias
- PMID: 35282836
- PMCID: PMC8919640
- DOI: 10.1186/s12872-022-02544-6
Conventional fluoroscopy-guided versus zero-fluoroscopy catheter ablation of supraventricular tachycardias
Abstract
Purpose: The aim of this study was to evaluate the safety and efficacy of zero-fluoroscopy (ZF) catheter ablation (CA) for supraventricular tachycardias (SVT).
Methods: 584 consecutive patients referred to our institution for CA of SVT were analysed. Patients were categorised into two groups; zero-fluoroscopy (ZF) group and conventional fluoroscopy (CF) group. The ZF group was further divided into two subgroups (adults and paediatric). Patient characteristics, procedural information, and follow-up data were compared.
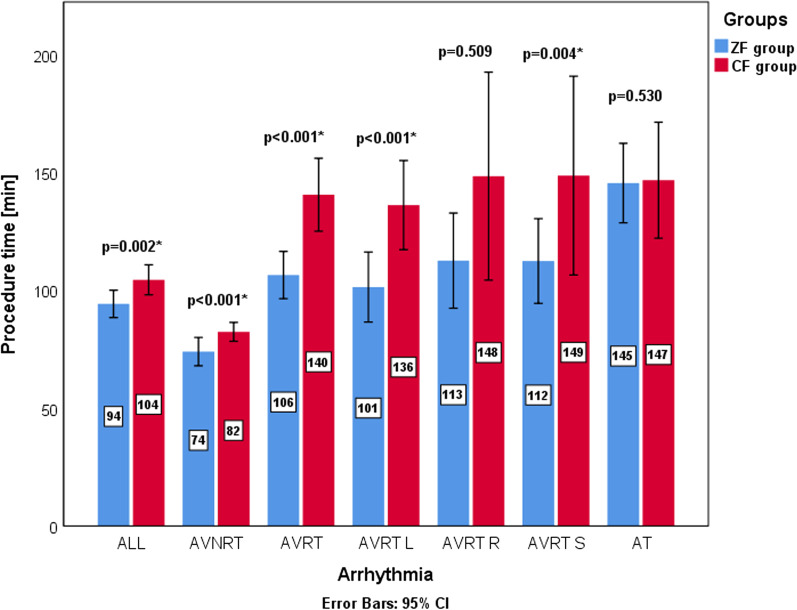
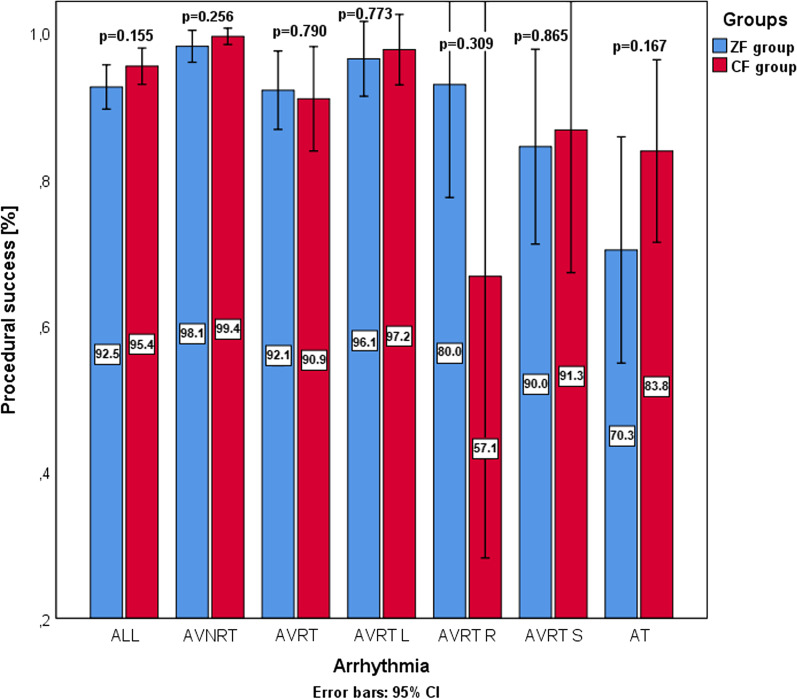
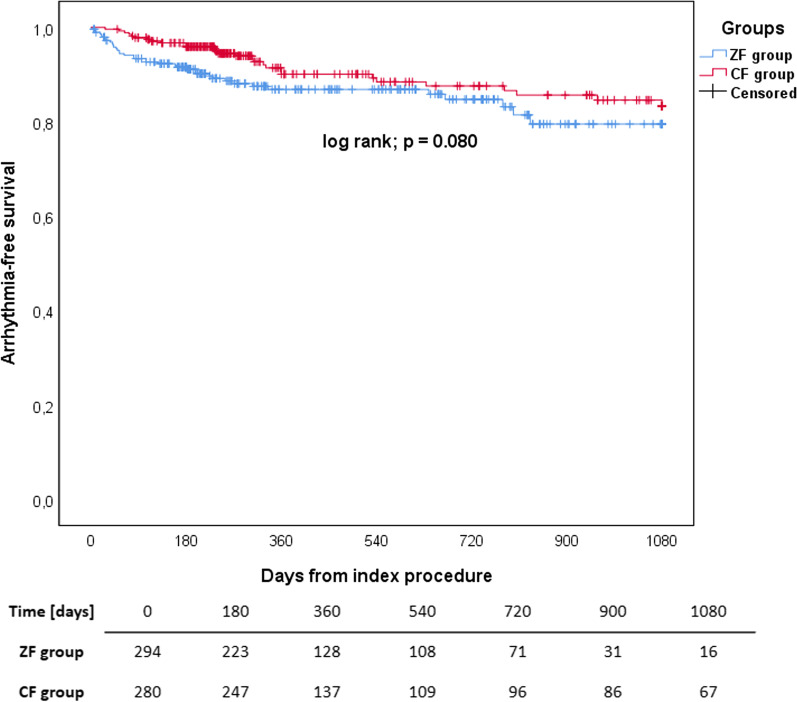
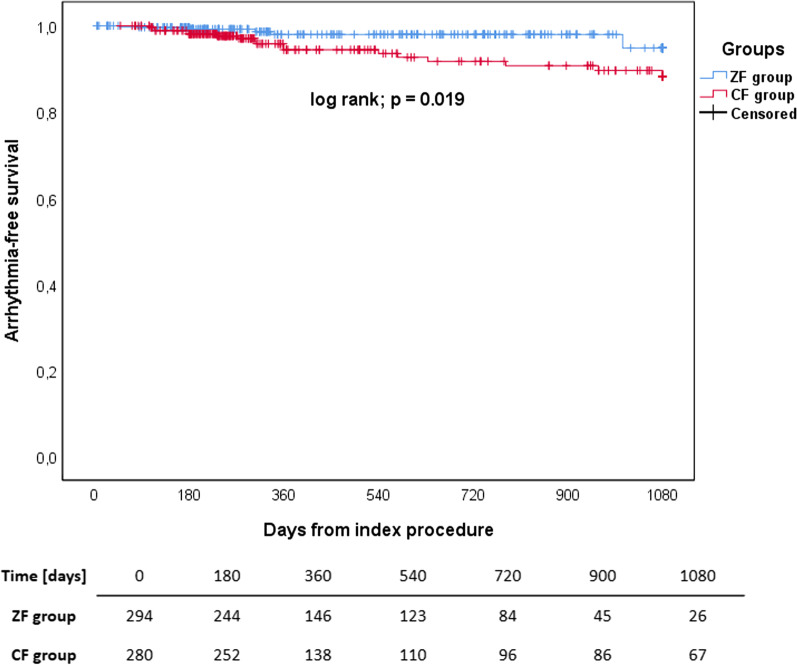
Results: The ZF group had a higher proportion of paediatric patients (42.2% vs 0.0%; p < 0.001), resulting in a younger age (30.9 ± 20.3 years vs 52.7 ± 16.5 years; p < 0.001) and lower BMI (22.8 ± 5.7 kg/m2 vs 27.0 ± 5.4 kg/m2; p < 0.001). Procedure time was shorter in the ZF group (94.2 ± 50.4 min vs 104.0 ± 54.0 min; p = 0.002). There were no major complications and the rate of minor complications did not differ between groups (0.0% vs 0.4%; p = 0.304). Acute procedural success as well as the long-term success rate when only the index procedure was considered did not differ between groups (92.5% vs 95.4%; p = 0.155; 87.1% vs 89.2%; p = 0.422). When repeated procedures were included, the long-term success rate was higher in the ZF group (98.3% vs 93.5%; p = 0.004). The difference can be partially explained by the operators' preferences.
Conclusion: The safety and efficacy of ZF procedures in adult and paediatric populations are comparable to that of CF procedures.
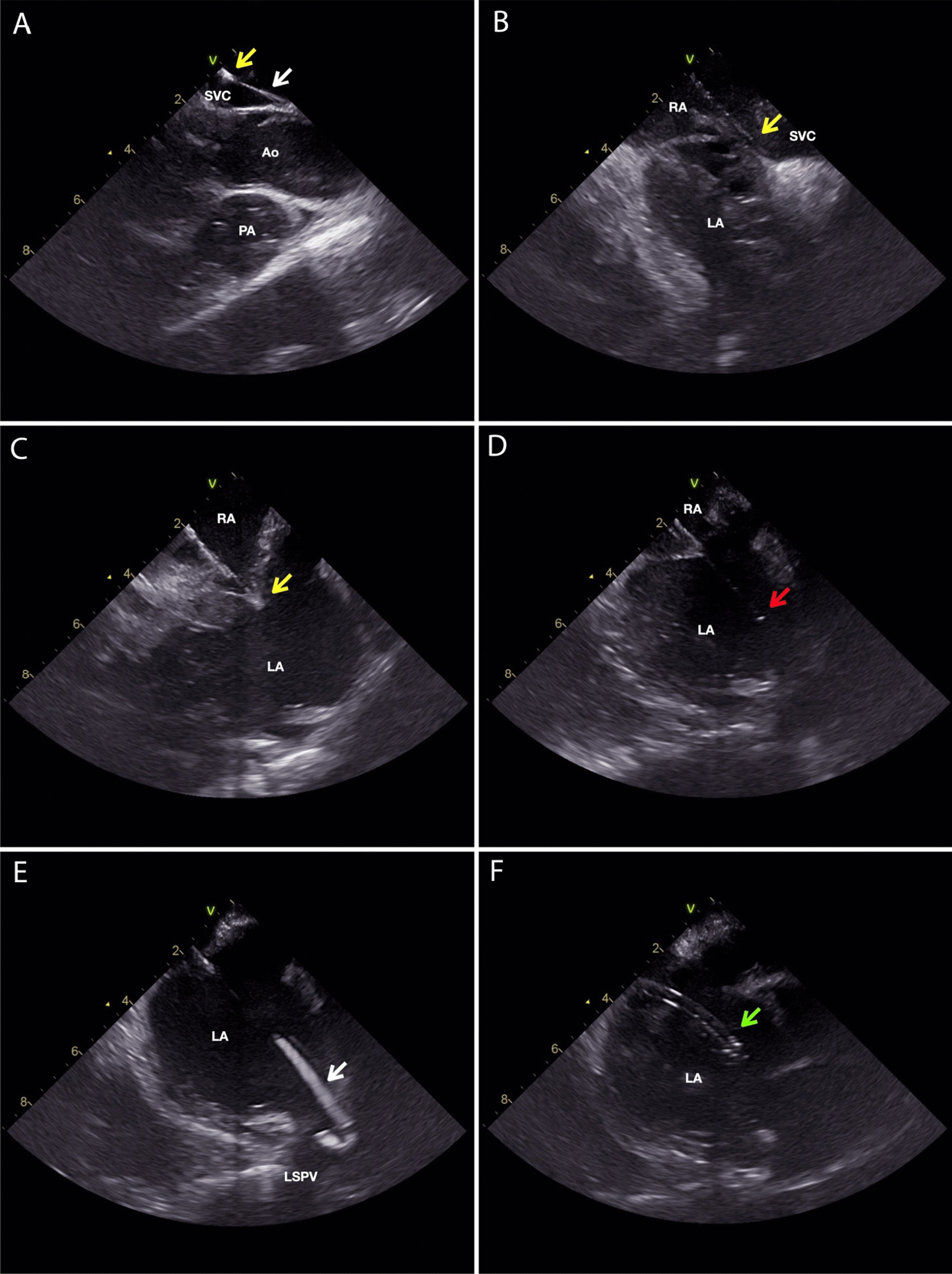
Keywords: Cryoablation; Intracardiac echocardiography; Paediatric population; Supraventricular tachycardia; Three-dimensional electroanatomic mapping system; Zero-fluoroscopy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Hirshfeld JW, Ferrari VA, Bengel FM, Bergersen L, Chambers CE, Einstein AJ, et al. 2018 ACC/HRS/NASCI/SCAI/SCCT Expert consensus document on optimal use of ionizing radiation in cardiovascular imaging—best practices for safety and effectiveness, part 2: radiological equipment operation, dose-sparing methodologies, patient and medical personnel. J Am Coll Cardiol. 2018;71:2829–2855. doi: 10.1016/j.jacc.2018.02.018. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
