

Clinical-Dermoscopic-Histopathological Correlations in Collision Skin Tumours
- PMID: 35283495
- PMCID: PMC8906304
- DOI: 10.4103/ijd.ijd_938_20
Clinical-Dermoscopic-Histopathological Correlations in Collision Skin Tumours
Abstract
Objectives: Collision tumours are rare situations characterised by the coincidence of two different skin neoplasms in the same lesion.
Methods: We have analyzed 41 collision skin tumours from one department in the clinical-dermoscopic-histopathologic correlations.
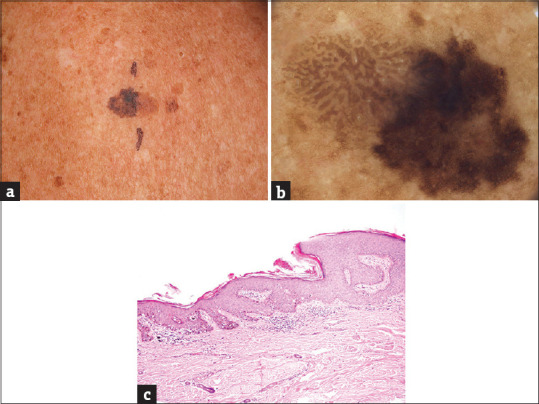
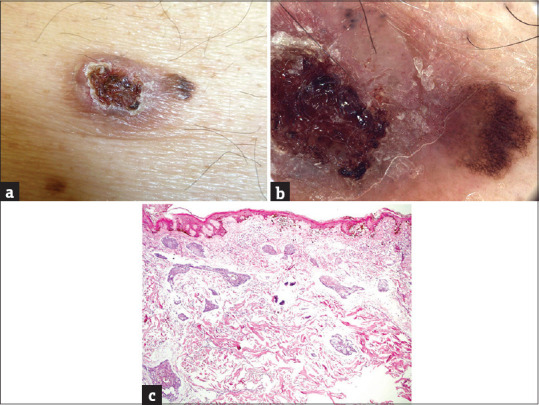
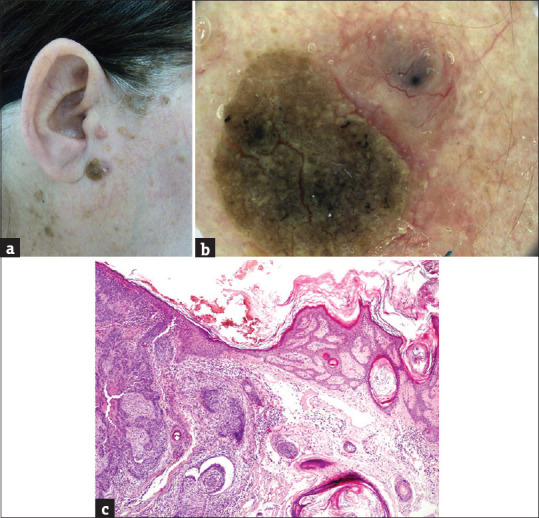
Results: We present 41 collisions tumours. The mean age of our patients was 67.9 years, the mean diameter of the lesion was 11.6 mm. The most frequent locations were trunk (27 lesions) and head/neck (11 lesions). The collisions were classified as benign/benign (13 cases), benign/malignant (25 cases) and malignant/malignant (3 cases). The most frequent participants were seborrheic keratosis (24 cases), malignant melanoma (17 cases), melanocytic nevus (14 cases), basal cell carcinoma (12 cases) and heamangioma (10 cases). Thirty cases were of "dominant/minor" type and 11 cases of "half to half" type. Malignant tumours were a part of 28 collisions; these lesions were larger, patients were older and the malignant part was dominant in most cases. More than half of the collisions were unexpected by the initial clinical examination. Six collisions were missed by the initial histopathological examination.
Conclusions: Collision tumours can be missed by clinical or even histopathological examination. Dermoscopy is very helpful in the recognizing of difficult cases and cooperating with the histopathologist.
Keywords: Collision tumor; dermoscopy; histopathology; malignant melanoma.
Copyright: © 2022 Indian Journal of Dermatology.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol. 2002;3:159–65. - PubMed
-
- Vestergaard ME, Macaskill P, Holt PE, Menzies SW. Dermoscopy compared with naked eye examination for the diagnosis of primary melanoma: A meta-analysis of studies performed in a clinical setting. Br J Dermatol. 2008;159:669–76. - PubMed
-
- Tognetti L, Cinotti E, Perrot JL, Campoli M, Fimiani M, Rubegni P. Benign and malignant collision tumors of melanocytic skin lesions with hemangioma: Dermoscopic and reflectance confocal microscopy features. Skin Res Technol. 2018;24:313–7. - PubMed
-
- Blum A, Maltagliati-Holzner P, Deinlein T, Hofmann-Wellenhof R. Collision tumors in dermoscopy: A new challenge. Hautarzt. 2018;69:776–9. - PubMed
LinkOut - more resources
Full Text Sources