

Probabilistic classification of anti-SARS-CoV-2 antibody responses improves seroprevalence estimates
- PMID: 35284072
- PMCID: PMC8891432
- DOI: 10.1002/cti2.1379
Probabilistic classification of anti-SARS-CoV-2 antibody responses improves seroprevalence estimates
Abstract
Objectives: Population-level measures of seropositivity are critical for understanding the epidemiology of an emerging pathogen, yet most antibody tests apply a strict cutoff for seropositivity that is not learnt in a data-driven manner, leading to uncertainty when classifying low-titer responses. To improve upon this, we evaluated cutoff-independent methods for their ability to assign likelihood of SARS-CoV-2 seropositivity to individual samples.
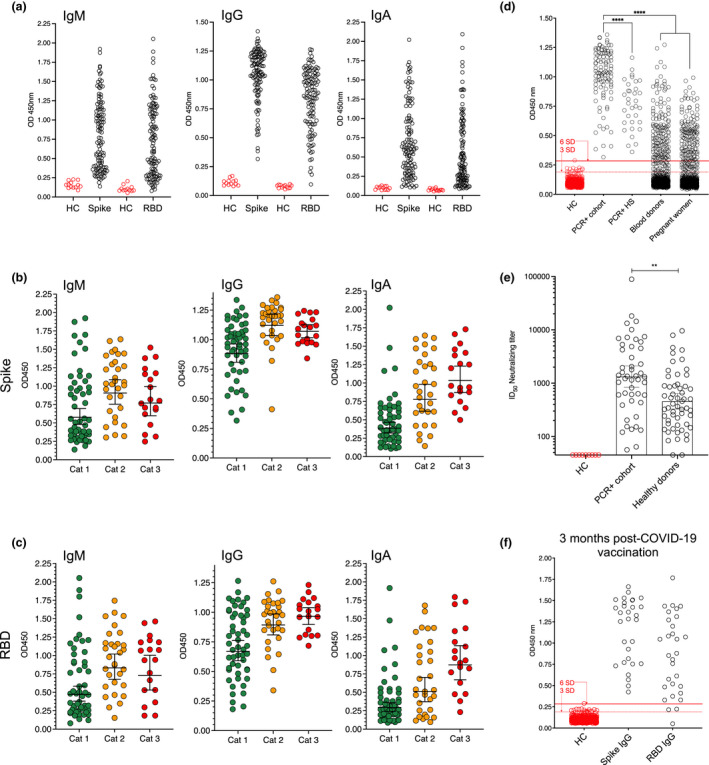
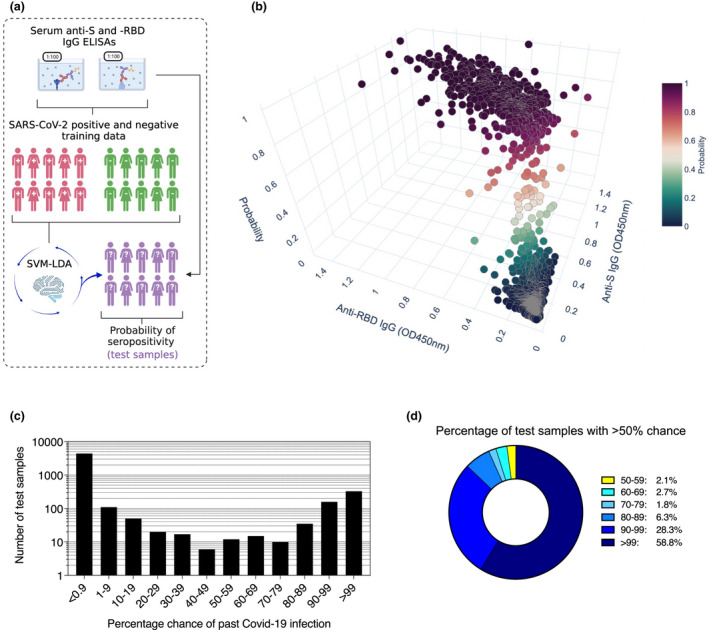
Methods: Using robust ELISAs based on SARS-CoV-2 spike (S) and the receptor-binding domain (RBD), we profiled antibody responses in a group of SARS-CoV-2 PCR+ individuals (n = 138). Using these data, we trained probabilistic learners to assign likelihood of seropositivity to test samples of unknown serostatus (n = 5100), identifying a support vector machines-linear discriminant analysis learner (SVM-LDA) suited for this purpose.
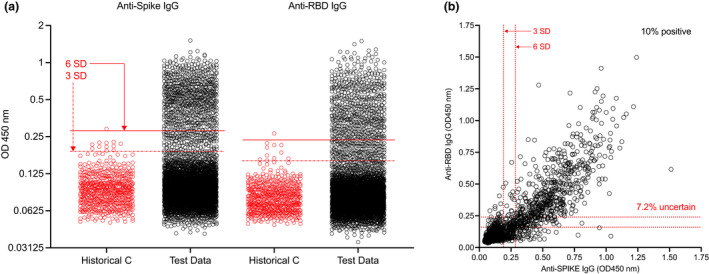
Results: In the training data from confirmed ancestral SARS-CoV-2 infections, 99% of participants had detectable anti-S and -RBD IgG in the circulation, with titers differing > 1000-fold between persons. In data of otherwise healthy individuals, 7.2% (n = 367) of samples were of uncertain serostatus, with values in the range of 3-6SD from the mean of pre-pandemic negative controls (n = 595). In contrast, SVM-LDA classified 6.4% (n = 328) of test samples as having a high likelihood (> 99% chance) of past infection, 4.5% (n = 230) to have a 50-99% likelihood, and 4.0% (n = 203) to have a 10-49% likelihood. As different probabilistic approaches were more consistent with each other than conventional SD-based methods, such tools allow for more statistically-sound seropositivity estimates in large cohorts.
Conclusion: Probabilistic antibody testing frameworks can improve seropositivity estimates in populations with large titer variability.
Keywords: COVID‐19; SARS‐CoV‐2; antibody responses; antibody testing; probability; serology.
© 2022 The Authors. Clinical & Translational Immunology published by John Wiley & Sons Australia, Ltd on behalf of Australian and New Zealand Society for Immunology, Inc.
Conflict of interest statement
The study authors declare no competing financial interests that could compromise the study. CW also receives funding from GlaxoSmithKline and Merck Sharp & Dohme; these funders had no role in the design, analysis or interpretation of this study. The views expressed are those of the authors.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous