

TIMP-1: A Circulating Biomarker for Pulmonary Hypertension Diagnosis Among Chronic Obstructive Pulmonary Disease Patients
- PMID: 35284430
- PMCID: PMC8914225
- DOI: 10.3389/fmed.2021.774623
TIMP-1: A Circulating Biomarker for Pulmonary Hypertension Diagnosis Among Chronic Obstructive Pulmonary Disease Patients
Abstract
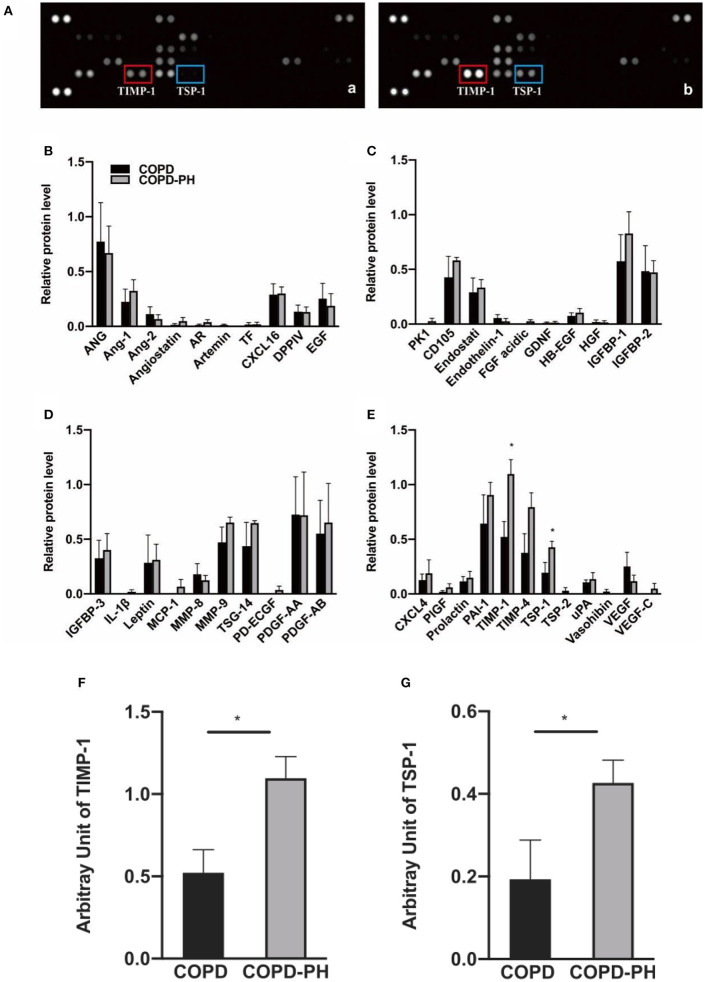
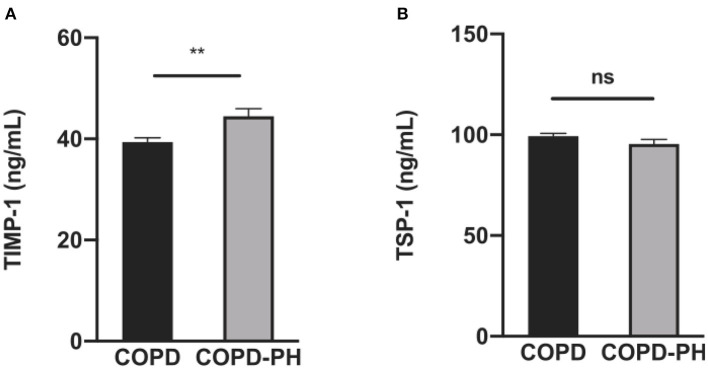
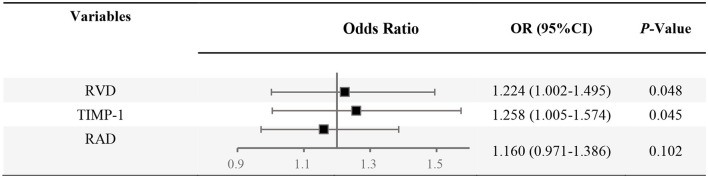
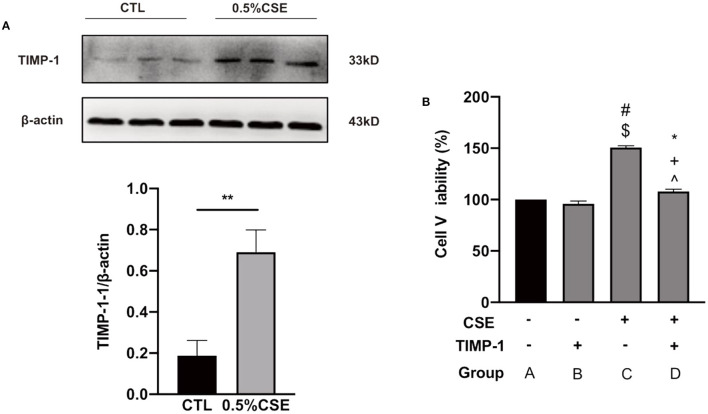
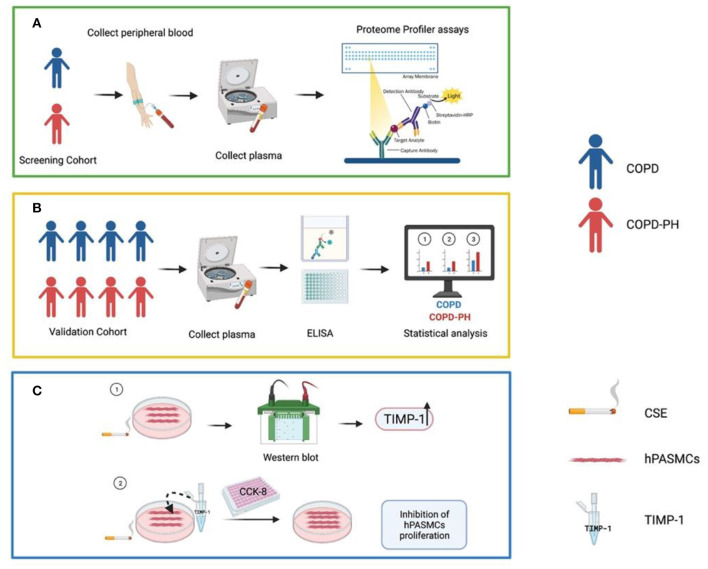
Pulmonary hypertension (PH) is a common complication of chronic obstructive pulmonary disease (COPD) and induces increased mortality among COPD patients. However, there are no blood biomarkers to identify PH in COPD. Here, we investigated whether circulating angiogenic factors and cytokines could serve as (a) biomarker (s) for COPD-PH patients. Using Angiogenesis and Cytokine proteome profile array assay, we measured the level of 36 cytokines and 55 angiogenesis-associated proteins in plasma from four COPD patients with PH (COPD-PH) and four COPD patients without PH (COPD), respectively, tissue inhibitor of metalloproteinase 1 (TIMP-1) and thrombospondin 1(TSP-1) were significantly different between the two groups. Enzyme-linked immunosorbent assay (ELISA) was applied to measured TIMP-1 and TSP-1 in a validation cohort (COPD-PH, n = 28; COPD, n = 18), and TIMP-1 was the only factor that was significantly different between COPD-PH and COPD patients (P < 0.01). Logistic regression analysis demonstrated that elevated TIMP-1 was an independent risk factor for COPD-PH [odds ratio (OR) = 1.258, 95% CI: 1.005-1.574, P < 0.05). Next, we explored the expression level and function of TIMP-1 in human pulmonary arterial smooth muscle cells (hPASMCs) exposed to cigarette smoking extract (CSE, a major etiological factor of COPD). In cultured hPASMCs, CSE treatment increased both TIMP-1 protein level and cell proliferation, and exogenous TIMP-1 (25 ng/mL) treatment inhibited CSE-induced hPASMCs proliferation. Overall, our results indicated that TIMP-1 elevation could serve as a circulating biomarker to diagnose PH among COPD patients, and TIMP-1 elevation in COPD-PH could be adaptive.
Keywords: TIMP-1; biomarker; chronic obstructive pulmonary disease; diagnosis; pulmonary hypertension.
Copyright © 2022 He, Liu, Liao, Liu, Lei, Wei, Ruan, Kunwar, Lu, Wang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous