

The Application of Scrotoscope-Assisted Minimally Invasive Excision for Epididymal Mass: An Initial Report
- PMID: 35284490
- PMCID: PMC8907580
- DOI: 10.3389/fsurg.2022.804803
The Application of Scrotoscope-Assisted Minimally Invasive Excision for Epididymal Mass: An Initial Report
Abstract
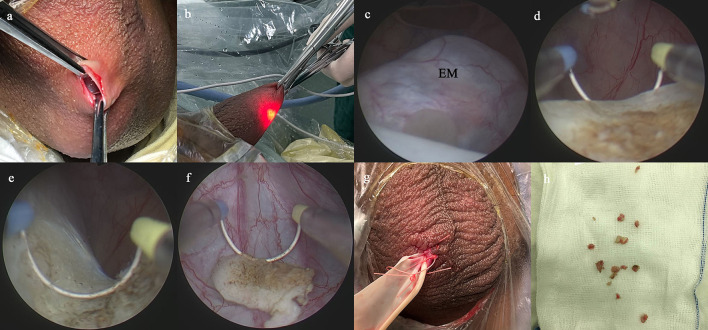
Background: To compare the middle-term efficacy and safety results between scrotoscope-assisted (SA) minimally invasive excision and traditional open excision (OE) for the treatment of epididymal mass.
Methods: A total of 253 males with surgery excision of epididymal mass from 2012 to 2018 were included in this retrospective study. Patients were divided into two groups: the traditional OE group and the SA group. Patient demographics and intraoperative and postoperative outcomes were obtained and compared between these two groups.
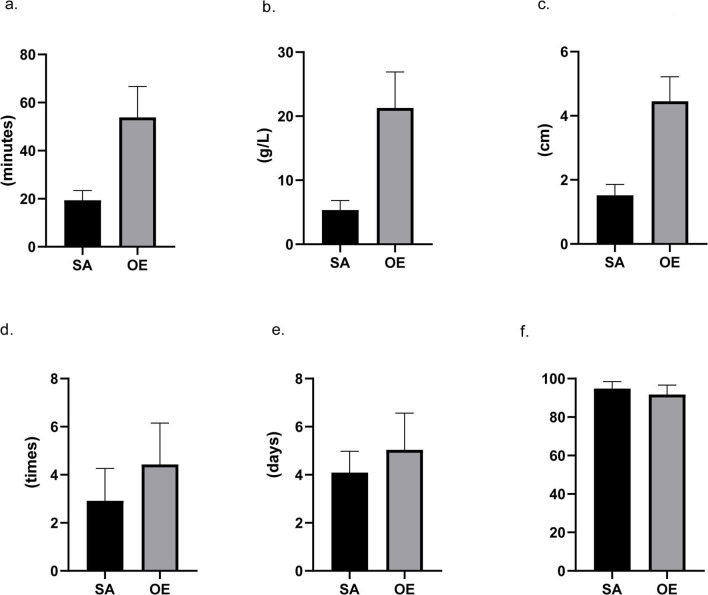
Results: About 174 patients (68.8%) underwent SA, and the other 79 (31.2%) underwent OE. Demographic data were similar between the two groups. Compared with OE surgery, SA could significantly shorten the operating time (19.4 ± 4.1 vs. 53.8 ± 12.9 min), reduce blood loss (5.3 ± 1.5 vs. 21.3 ± 5.6 ml), and downsize the operative incision (1.5 ± 0.3 vs. 4.5 ± 0.8 cm). Additionally, postoperative complications were significantly less occurred in the SA group than those in OE (15.5% vs. 21.5%), in particular scrotal hematoma (1.7% vs. 12.7%) and incision discomfort (2.8% vs. 6.3%). Patients in the SA group had a significantly higher overall satisfaction score (94.8 ± 3.7 vs. 91.7 ± 4.9) and a significantly shorter length of hospital stay (4.1 ± 0.9 vs. 5.0 ± 1.5 days) than those in the OE group. No postoperative testicular atrophy occurred in the SA group.
Conclusion: SA is emerging as a novel and effective option with promising perspectives for epididymal mass therapy.
Keywords: epididymal mass; minimally invasive; open excision; scrotal disease; scrotoscope.
Copyright © 2022 Qin, Yang, Zhang, Yang, Cai, Li, Zhu, Ye, Gao and Wei.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources