

Liver resection versus liver transplantation for hepatocellular carcinoma within Milan criteria: a meta-analysis of 18,421 patients
- PMID: 35284509
- PMCID: PMC8847852
- DOI: 10.21037/hbsn-21-350
Liver resection versus liver transplantation for hepatocellular carcinoma within Milan criteria: a meta-analysis of 18,421 patients
Abstract
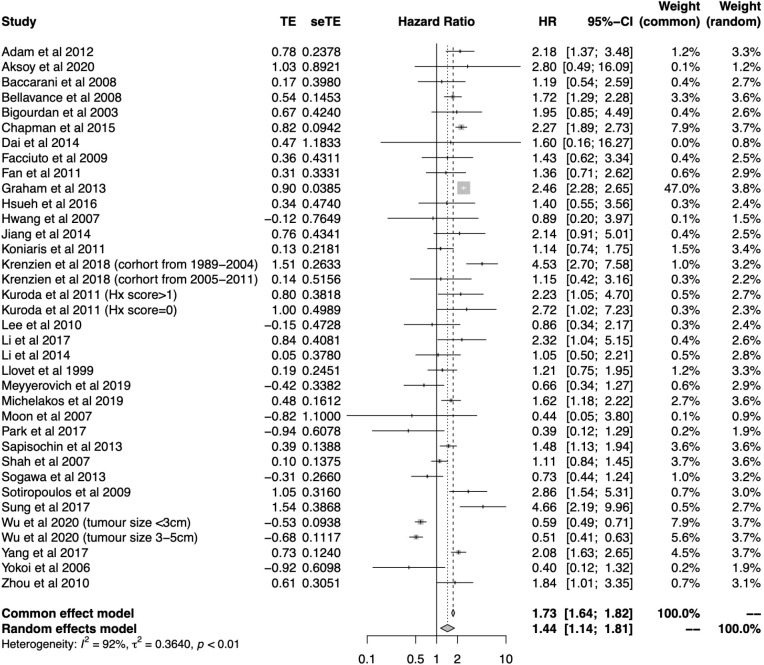
Background: Outcomes after liver resection (LR) and liver transplantation (LT) for hepatocellular carcinoma (HCC) are heterogenous and may vary by region, over time periods and disease burden. We aimed to compare overall survival (OS) and disease-free survival (DFS) between LT versus LR for HCC within the Milan criteria.
Methods: Two authors independently searched Medline and Embase databases for studies comparing survival after LT and LR for patients with HCC meeting the Milan criteria. Meta-analyses and metaregression were conducted using random-effects models.
Results: We screened 2,278 studies and included 35 studies with 18,421 patients. LR was associated with poorer OS [hazard ratio (HR) =1.44; 95% confidence interval (CI): 1.14-1.81; P<0.01] and DFS (HR =2.71; 95% CI: 2.23-3.28; P<0.01) compared to LT, with similar findings among intention-to-treat (ITT) studies. In uninodular disease, OS in LR was comparable to LT (P=0.13) but DFS remained poorer (HR =2.95; 95% CI: 2.30-3.79; P<0.01). By region, LR had poorer OS versus LT in North America and Europe (P≤0.01), but not Asia (P=0.25). LR had inferior survival versus LT in studies completed before 2010 (P=0.01), but not after 2010 (P=0.12). Cohorts that underwent enhanced surveillance had comparable OS after LT and LR (P=0.33), but cohorts undergoing usual surveillance had worse OS after LR (HR =1.95; 95% CI: 1.24-3.07; P<0.01).
Conclusions: Mortality after LR for HCC is nearly 50% higher compared to LT. Survival between LR and LT were similar in uninodular disease. The risk of recurrence after LR is threefold that of LT.
Keywords: Hepatocellular carcinoma (HCC); liver resection (LR); liver transplant; recurrence; survival.
2022 Hepatobiliary Surgery and Nutrition. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://hbsn.amegroups.com/article/view/10.21037/hbsn-21-350/coif). The authors have no conflicts of interest to declare.
Figures



Comment in
-
Is liver transplantation superior to liver resection for hepatocellular carcinoma within Milan criteria?Hepatobiliary Surg Nutr. 2022 Aug;11(4):645-646. doi: 10.21037/hbsn-22-196. Hepatobiliary Surg Nutr. 2022. PMID: 36016729 Free PMC article. No abstract available.
-
Resection vs. transplantation for hepatocellular carcinoma: a never ending challenge.Hepatobiliary Surg Nutr. 2023 Jun 1;12(3):443-446. doi: 10.21037/hbsn-23-131. Epub 2023 May 8. Hepatobiliary Surg Nutr. 2023. PMID: 37351126 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources