

Associating liver partition and portal vein ligation for staged hepatectomy versus sequential transarterial chemoembolization and portal vein embolization in staged hepatectomy for HBV-related hepatocellular carcinoma: a randomized comparative study
- PMID: 35284529
- PMCID: PMC8847855
- DOI: 10.21037/hbsn-20-264
Associating liver partition and portal vein ligation for staged hepatectomy versus sequential transarterial chemoembolization and portal vein embolization in staged hepatectomy for HBV-related hepatocellular carcinoma: a randomized comparative study
Abstract
Background: Both portal vein embolization (PVE) and associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) have merits and demerits when used in patients with unresectable liver cancers due to insufficient volumes in future liver remnant (FLR).
Methods: This study was a single-center, prospective randomized comparative study. Patients with the diagnosis of hepatitis B related hepatocellular carcinoma (HCC) were randomly assigned in a 1:1 ratio to the 2 groups. The primary endpoints were tumor resection and three-year overall survival (OS) rates.
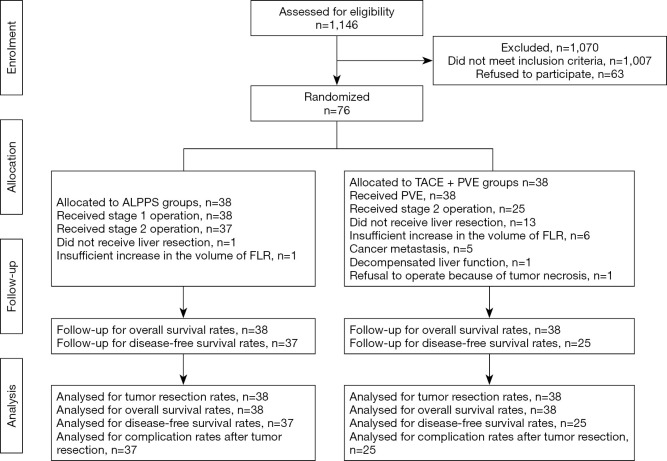
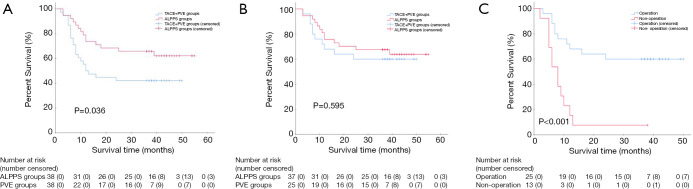
Results: Between November 2014 to June 2016, 76 patients with unresectable HBV-related HCC due to inadequate volume of FLR were randomly assigned to ALPPS groups (n=38) and TACE + PVE groups (n=38). Thirty-seven patients (97.4%) in the ALPPS group compared with 25 patients (65.8%) in the TACE + PVE group were able to undergo staged hepatectomy (risk ratio 1.48, 95% CI: 1.17-1.87, P<0.001). The three-year OS rate of the ALPPS group (65.8%) (95% CI: 50.7-80.9) was significantly better than the TACE + PVE group (42.1%) (95% CI: 26.4-57.8) (HR 0.50, 95% CI: 0.26-0.98, two-sided P=0.036). However, no significant difference in the OS rates between patients who underwent tumor resection in the 2 groups of patients was found (HR 0.80, 95% CI: 0.35-1.83, two-sided P=0.595). Major postoperative complications rates after the stage-2 hepatectomy were 54.1% in the ALPPS group and 20.0% in the TACE + PVE group (risk ratio 2.70, 95% CI: 1.17-6.25, P=0.007).
Conclusions: ALPPS resulted in significantly better intermediate-term OS outcomes, at the expenses of a significantly higher perioperative morbidity rate compared with TACE + PVE in patients who had initially unresectable HBV-related HCC.
Keywords: Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS); hepatocellular carcinoma (HCC); portal vein embolization (PVE); prognosis; resection rate.
2022 Hepatobiliary Surgery and Nutrition. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://hbsn.amegroups.com/article/view/10.21037/hbsn-20-264/coif). WPZ reports grants from NSFC, China, grants from State Key Infection Disease Project of China, grants from National Human Genetic Resources Sharing Service Platform, during the conduct of the study. The other authors have no conflicts of interest to declare.
Figures
Comment in
-
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS)-a fine balance.Hepatobiliary Surg Nutr. 2023 Apr 10;12(2):269-271. doi: 10.21037/hbsn-23-96. Epub 2023 Mar 15. Hepatobiliary Surg Nutr. 2023. PMID: 37124686 Free PMC article. No abstract available.
-
ALPPS versus portal vein embolization for hepatitis B virus-associated hepatocellular carcinoma: a delicate balance between volume and morbidity.Hepatobiliary Surg Nutr. 2023 Apr 10;12(2):284-286. doi: 10.21037/hbsn-23-119. Epub 2023 Mar 29. Hepatobiliary Surg Nutr. 2023. PMID: 37124693 Free PMC article. No abstract available.
-
Associating liver partition and portal vein ligation or combined transarterial chemo-embolisation and portal vein embolisation for staged hepatectomy for HBV-related hepatocellular carcinoma.Hepatobiliary Surg Nutr. 2023 Apr 10;12(2):272-275. doi: 10.21037/hbsn-23-101. Epub 2023 Mar 15. Hepatobiliary Surg Nutr. 2023. PMID: 37124694 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Miscellaneous