

Non-targeted metabonomic analysis of plasma in patients with atherosclerosis by liquid chromatography-mass spectrometry
- PMID: 35284547
- PMCID: PMC8905000
- DOI: 10.21037/atm-22-118
Non-targeted metabonomic analysis of plasma in patients with atherosclerosis by liquid chromatography-mass spectrometry
Abstract
Background: This study sought to analyze non-targeted plasma metabolites in patients with atherosclerosis (AS).
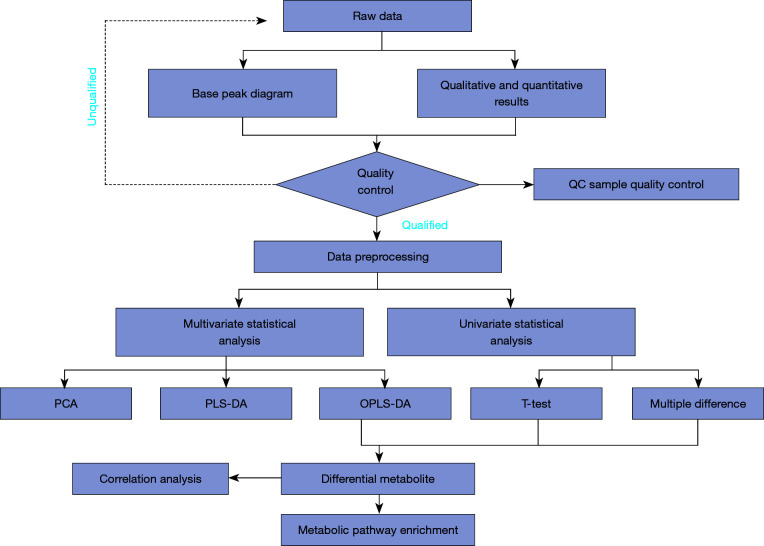
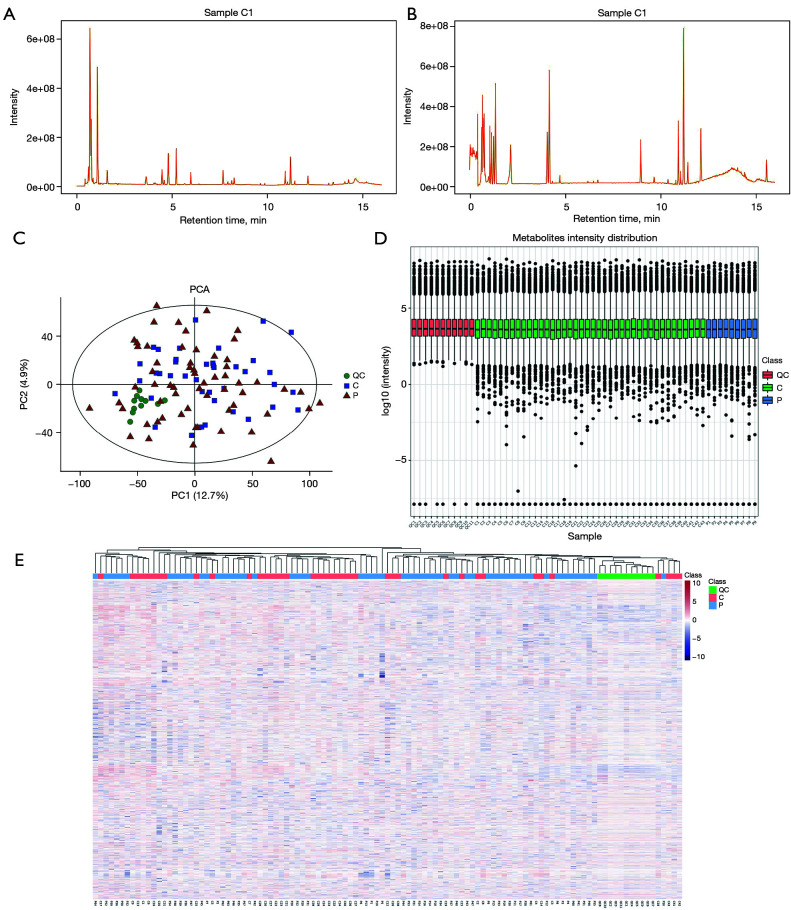
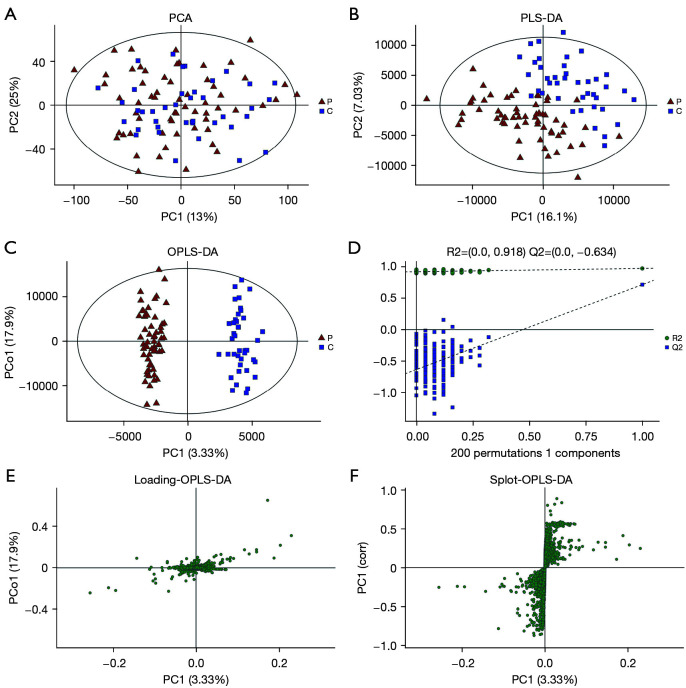
Methods: The plasma of patients with AS (the patient group) and the plasma of age-matched and gender-matched healthy individuals (the control group) at the Taihe Hospital was collected. One hundred patients were included in the study (60 in the patient group and 40 in the control group). Fasting venous plasma was collected in the morning. The metabolites in the plasma were examined by liquid chromatography-mass spectrometry (LC-MS). An unsupervised principal component analysis (PCA) was conducted to observe the overall distribution of each sample and the stability of the analysis process. Next, a supervised partial least squares-discriminant analysis (PLS-DA) and an orthogonal partial least squares-discriminant analysis (OPLS-DA) were conducted to examine the overall differences among the metabolic profiles of the groups and identify different metabolites in the groups. Pathway enrichment was analyzed using the Kyoto Encyclopedia of Genes and Genomes (KEGG) database.
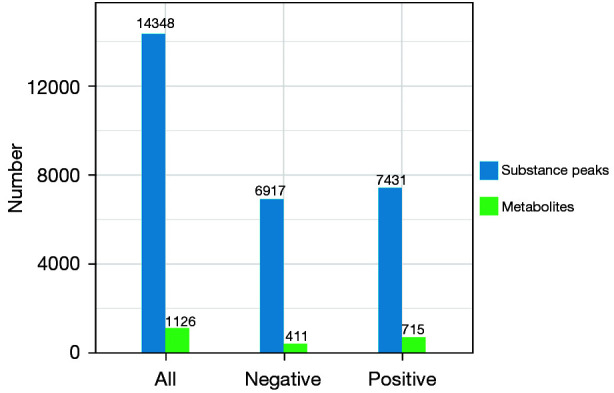
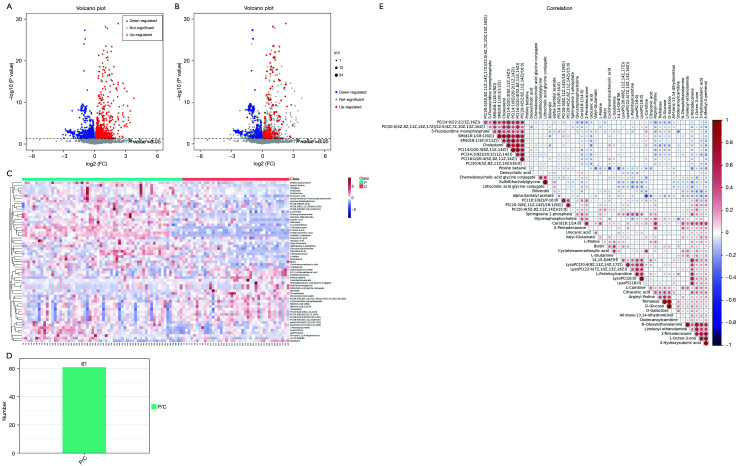
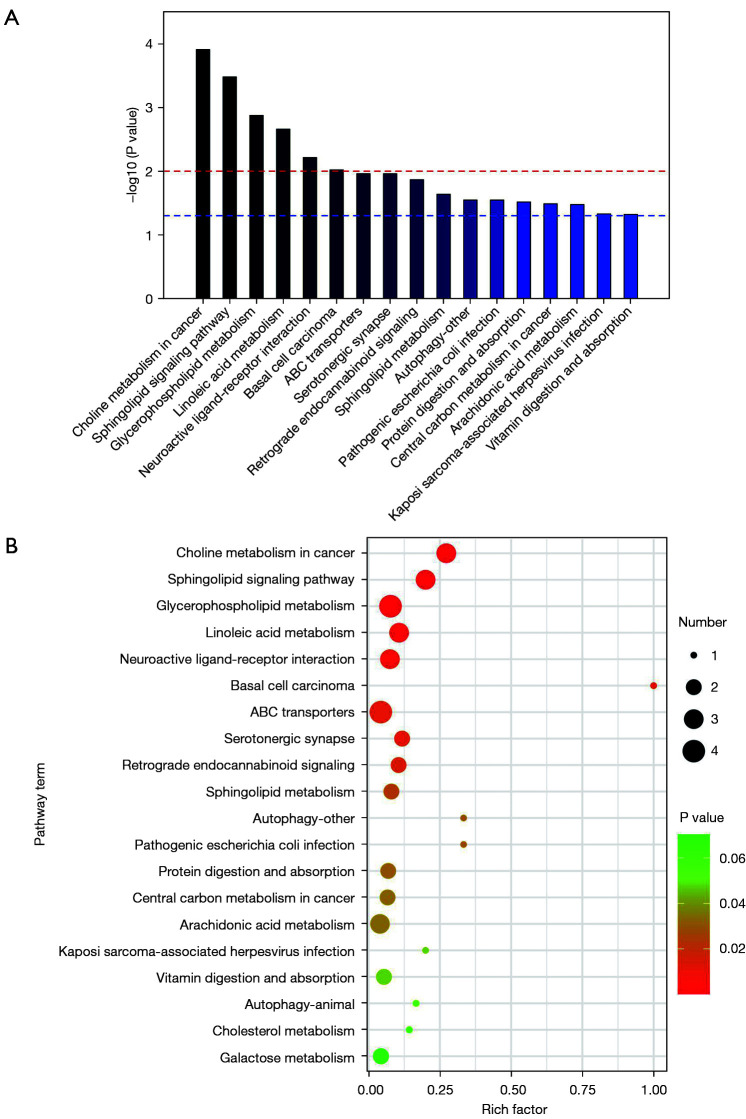
Results: In total, 1,126 different metabolites were detected in the patient and control groups. Compared to the control group, 411 species decreased, and 715 species increased in the patient group. There were 61 different metabolites with a variable weight in the projection (VIP) >1 and a P<0.05. There were 34 types of lipid metabolites, 10 types of carbon and oxygen compounds, 8 types of organic acids and derivatives, 4 types of organoheterocyclic compounds, 3 types of nitrogen-containing organic compounds, and 2 types of nucleotides and analogs. Compared to the control group, 47 species decreased, and 14 species increased in the patient group. The following 9 metabolites had the most significant differences (|log2fold change| >1; P<0.05): 2-tetradecanone, pantothenol, all-trans-13,14-dihydroretinol, linoleoyl ethanolamide, N-oleoylethanolamine, 4-methyl-2-pentenal, Cer (d18:1/14:0), chenodeoxycholic acid glycine conjugate, and 5-acetamidovalerate. The enrichment analysis results of the 61 different metabolite pathways identified 17 metabolic pathways with significant differences (P<0.05), including the choline metabolism, lipid metabolism, autophagy, amino acid metabolism, vitamin digestion, and absorption pathways.
Conclusions: There are significant differences in non-targeted plasma metabolites between patients with AS and healthy individuals. The above-mentioned 9 most significantly different metabolites may be potential markers of AS.
Keywords: Atherosclerosis (AS); difference metabolite; liquid chromatography-mass spectrometry (LC-MS) metabonomics; metabolic pathway.
2022 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-22-118/coif). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials