

Transient Middle Cerebral Artery Occlusion with an Intraluminal Suture Enables Reproducible Induction of Ischemic Stroke in Mice
- PMID: 35284595
- PMCID: PMC8857907
- DOI: 10.21769/BioProtoc.4305
Transient Middle Cerebral Artery Occlusion with an Intraluminal Suture Enables Reproducible Induction of Ischemic Stroke in Mice
Abstract
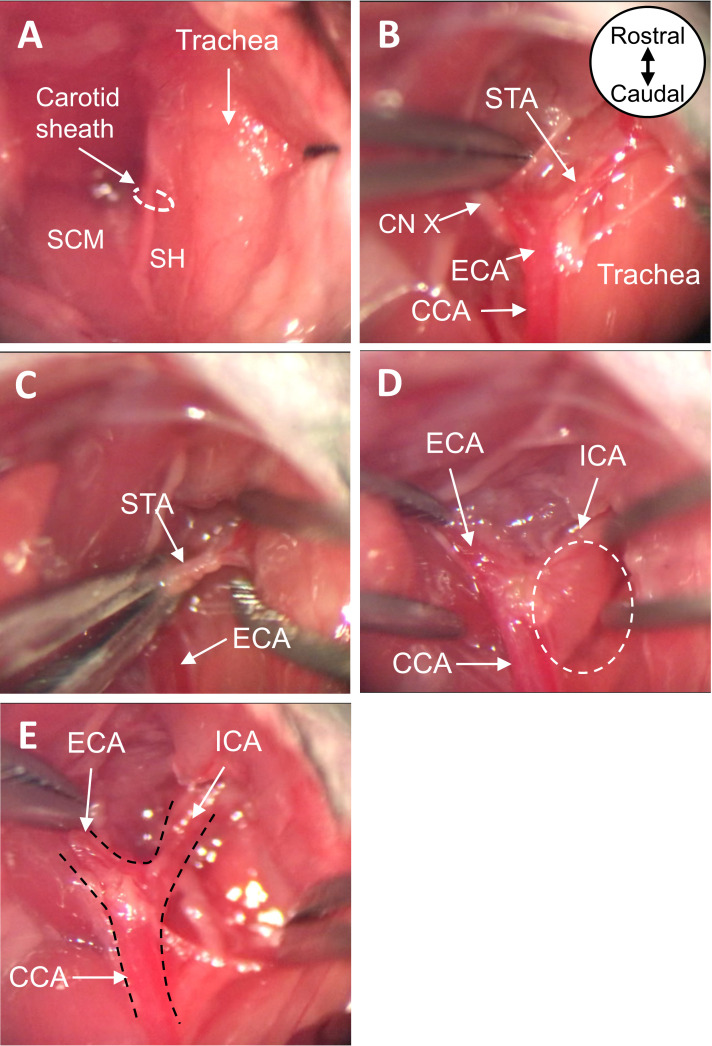
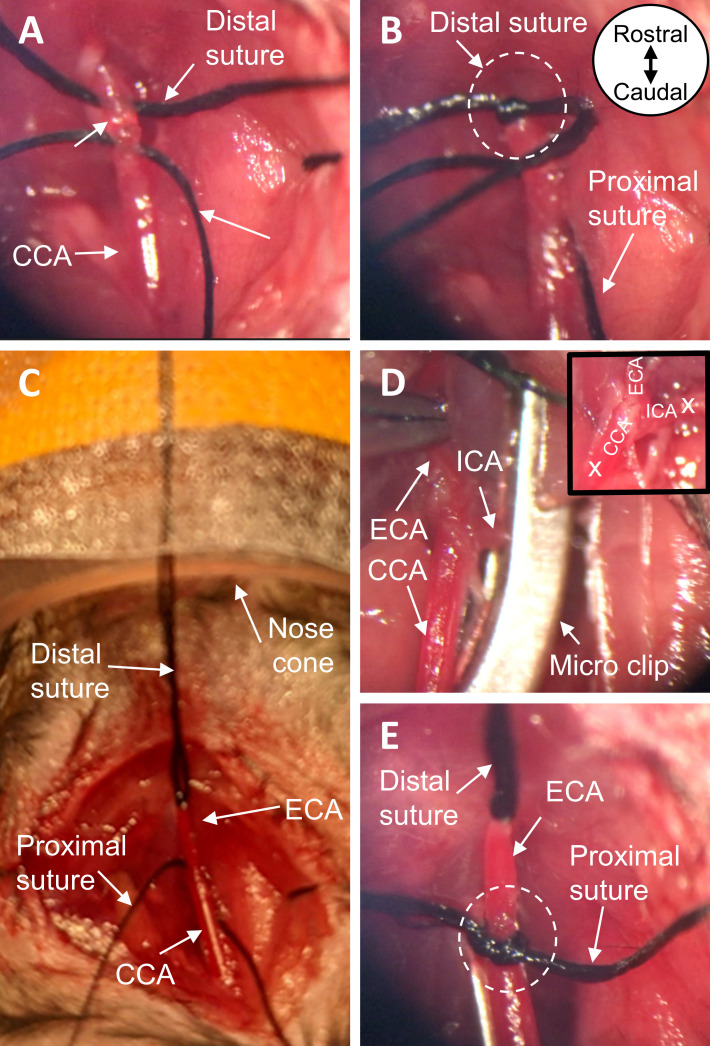
Ischemic stroke is a leading cause of mortality and chronic disability worldwide, underscoring the need for reliable and accurate animal models to study this disease's pathology, molecular mechanisms of injury, and treatment approaches. As most clinical strokes occur in regions supplied by the middle cerebral artery (MCA), several experimental models have been developed to simulate an MCA occlusion (MCAO), including transcranial MCAO, micro- or macro-sphere embolism, thromboembolisation, photothrombosis, Endothelin-1 injection, and - the most common method for ischemic stroke induction in murine models - intraluminal MCAO. In the intraluminal MCAO model, the external carotid artery (ECA) is permanently ligated, after which a partially-coated monofilament is inserted and advanced proximally to the common carotid artery (CCA) bifurcation, before being introduced into the internal carotid artery (ICA). The coated tip of the monofilament is then advanced to the origin of the MCA and secured for the duration of occlusion. With respect to other MCAO models, this model offers enhanced reproducibility regarding infarct volume and cognitive/functional deficits, and does not require a craniotomy. Here, we provide a detailed protocol for the surgical induction of unilateral transient ischemic stroke in mice, using the intraluminal MCAO model. Graphic abstract: Overview of the intraluminal monofilament method for transient middle cerebral artery occlusion (MCAO) in mouse.
Keywords: Brain reperfusion; Cerebral infarct; Intraluminal MCAO; Murine model; Rodent model; Transient MCAO.
Copyright © 2022 The Authors; exclusive licensee Bio-protocol LLC.
Conflict of interest statement
Competing interestsNo potential competing interest was reported by the authors.
Figures




References
-
- Barber P. A., Hoyte L., Colbourne F. and Buchan A. M.(2004). Temperature-regulated model of focal ischemia in the mouse: a study with histopathological and behavioral outcomes. Stroke 35(7): 1720-1725. - PubMed
-
- Benjamin E. J., Muntner P., Alonso A., Bittencourt M. S., Callaway C. W., Carson A. P., Chamberlain A. M., Chang A. R., Cheng S., Das S. R., et al. .(2019). Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 139(10): e56-e528. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
