

Feasibility of critical care ergometry: Exercise data of patients on mechanical ventilation analyzed as nine-panel plots
- PMID: 35285178
- PMCID: PMC8918698
- DOI: 10.14814/phy2.15213
Feasibility of critical care ergometry: Exercise data of patients on mechanical ventilation analyzed as nine-panel plots
Abstract
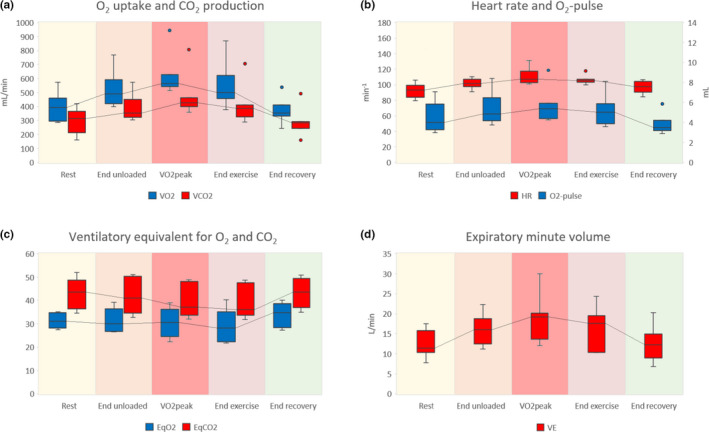
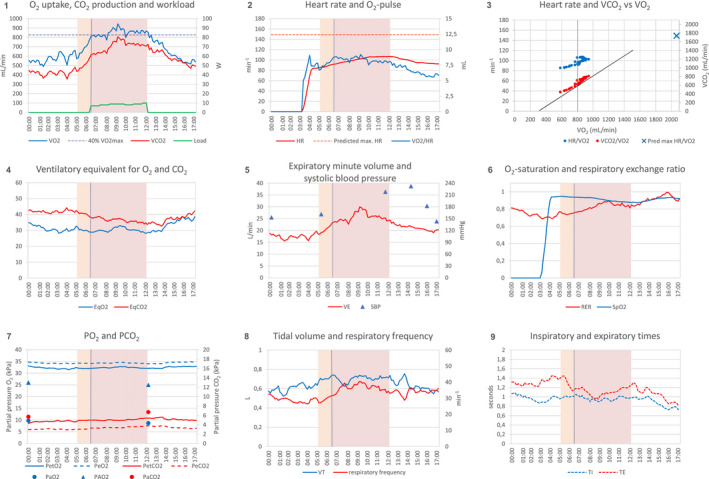
Nine-panel plots are standard displays of cardiopulmonary exercise data, used in cardiac and pulmonary medicine to investigate the nature of exercise limitation. We explored whether this approach could be used to analyze the data of critically ill patients on mechanical ventilation, capable of exercising actively. Patients followed an incremental exercise protocol using a bedside cycle ergometer. Respiratory gases were analyzed using indirect calorimetry, and blood gases were sampled from arterial catheters. Data of seven patients were combined into nine-panel plots. Systematic analysis clarified the nature of exercise limitation in six cases. Resting metabolic rate was increased in all patients, with a median oxygen uptake ( ) of 5.52 (IQR 4.29-6.31) ml/kg/min. Unloaded cycling increased the by 19.8% to 6.61 (IQR 5.99-7.08) ml/kg/min. Adding load to the ergometer increased the by another 20.0% to reach at a median of 7.14 (IQR 6.67-10.75) ml/kg/min, corresponding to a median extrinsic workload of 7 W. This was accompanied by increased CO2 production, respiratory minute volume, heart rate, and oxygen pulse. Three patients increased their to >40% of predicted , two patients passed the anaerobic threshold. Dead space ventilation was 44%, decreasing to 42% and accompanied by lower ventilatory equivalents during exercise. Exercise produced no net change in alveolo-arterial PO2 difference. We concluded that diagnostic ergometry in mechanically ventilated patients was feasible. Analysis of the data as nine-panel plots provided insight into individual limitations to exercise.
Keywords: circulation; critical care; exercise physiology; mechanical ventilation; oxygen consumption.
© 2022 The Authors. Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society.
Conflict of interest statement
None of the authors has any conflicting interests.
Figures
References
-
- Ainsworth, B. E. , Haskell, W. L. , Herrmann, S. D. , Meckes, N. , Bassett, D. R. , Tudor‐Locke, C. , Greer, J. L. , Vezina, J. , Whitt‐Glover, M. C. , & Leon, A. S. (2011). Compendium of physical activities: A second update of codes and MET values. Medicine and Science in Sports and Exercise, 43, 1575–1581. 10.1249/MSS.0b013e31821ece12 - DOI - PubMed
-
- Akoumianaki, E. , Dousse, N. , Lyazidi, A. , Lefebvre, J. C. , Graf, S. , Cordioli, R. L. , Rey, N. , Richard, J. M. , & Brochard, L. (2017). Can proportional ventilation modes facilitate exercise in critically ill patients? A physiological cross‐over study: Pressure support versus proportional ventilation during lower limb exercise in ventilated critically ill patients. Annals of Intensive Care, 7, 64. 10.1186/s13613-017-0289-y - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
