

Paraspinal Muscle in Chronic Low Back Pain: Comparison Between Standard Parameters and Chemical Shift Encoding-Based Water-Fat MRI
- PMID: 35285561
- PMCID: PMC9470775
- DOI: 10.1002/jmri.28145
Paraspinal Muscle in Chronic Low Back Pain: Comparison Between Standard Parameters and Chemical Shift Encoding-Based Water-Fat MRI
Abstract
Background: Paraspinal musculature (PSM) is increasingly recognized as a contributor to low back pain (LBP), but with conventional MRI sequences, assessment is limited. Chemical shift encoding-based water-fat MRI (CSE-MRI) enables the measurement of PSM fat fraction (FF), which may assist investigations of chronic LBP.
Purpose: To investigate associations between PSM parameters from conventional MRI and CSE-MRI and between PSM parameters and pain.
Study type: Prospective, cross-sectional.
Population: Eighty-four adults with chronic LBP (44.6 ± 13.4 years; 48 males).
Field strength/sequence: 3-T, T1-weighted fast spin-echo and iterative decomposition of water and fat with echo asymmetry and least squares estimation sequences.
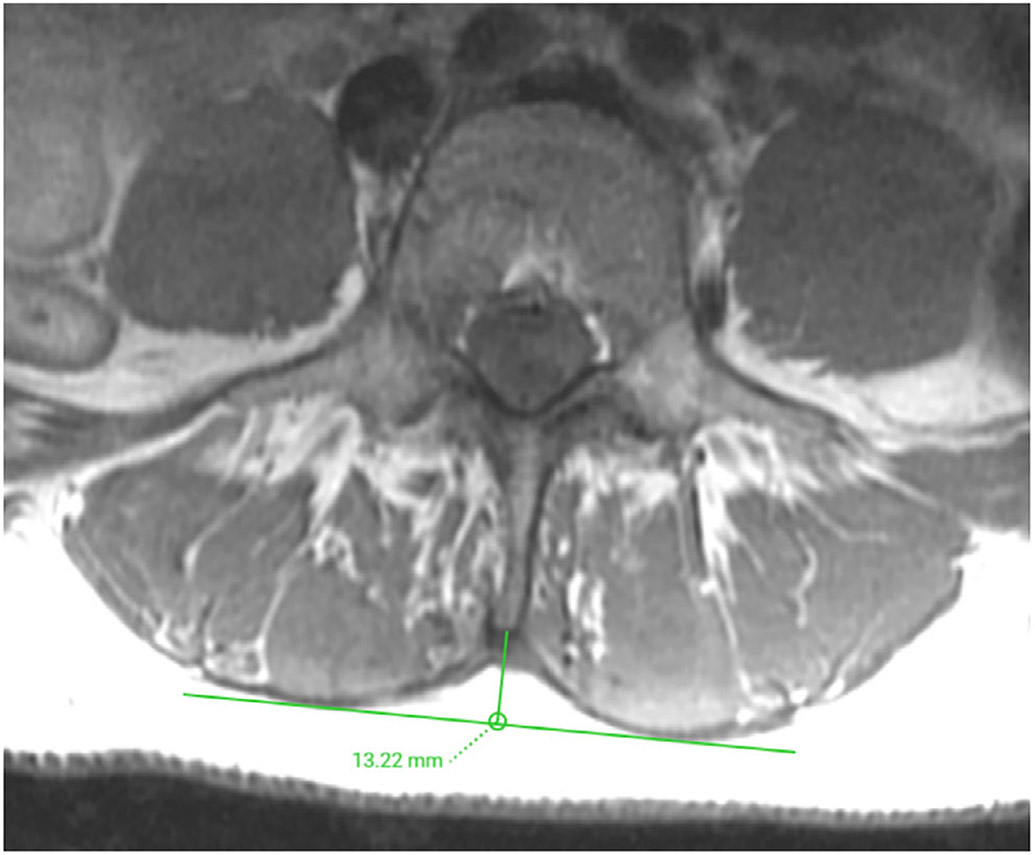
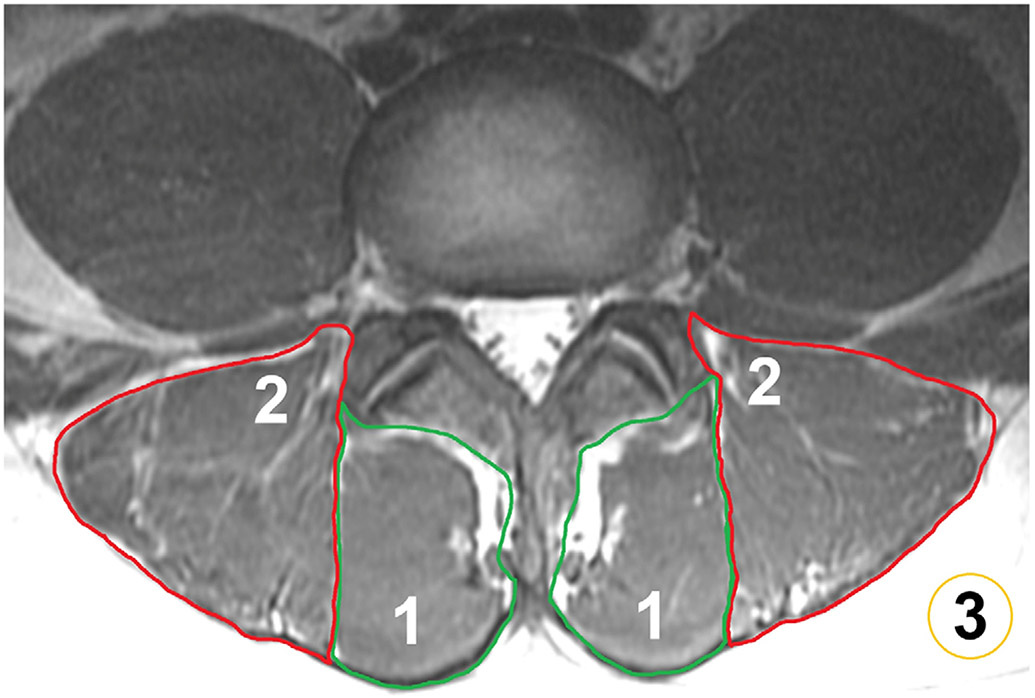
Assessment: T1-weighted images for Goutallier classification (GC), muscle volume, lumbar indentation value, and muscle-fat index, CSE-MRI for FF extraction (L1/2-L5/S1). Pain was self-reported using a visual analogue scale (VAS). Intra- and/or interreader agreement was assessed for MRI-derived parameters.
Statistical tests: Mixed-effects and linear regression models to 1) assess relationships between PSM parameters (entire cohort and subgroup with GC grades 0 and 1; statistical significance α = 0.0025) and 2) evaluate associations of PSM parameters with pain (α = 0.05). Intraclass correlation coefficients (ICCs) for intra- and/or interreader agreement.
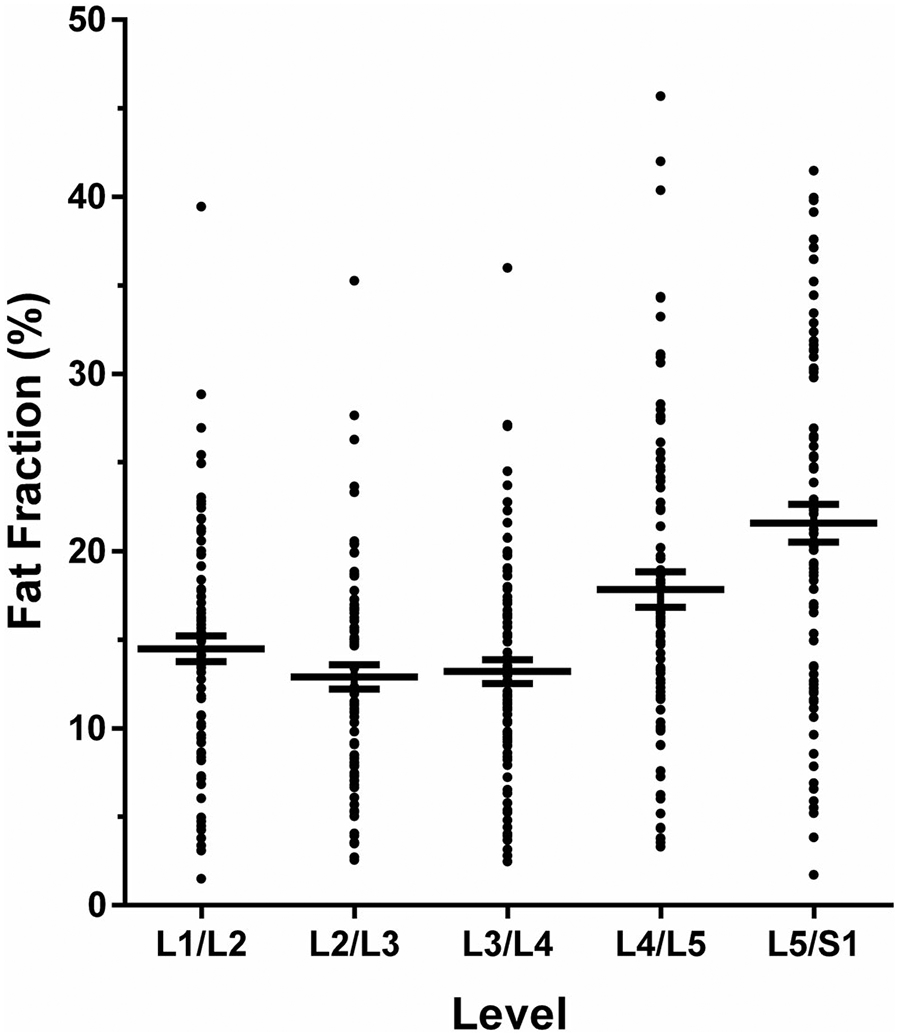
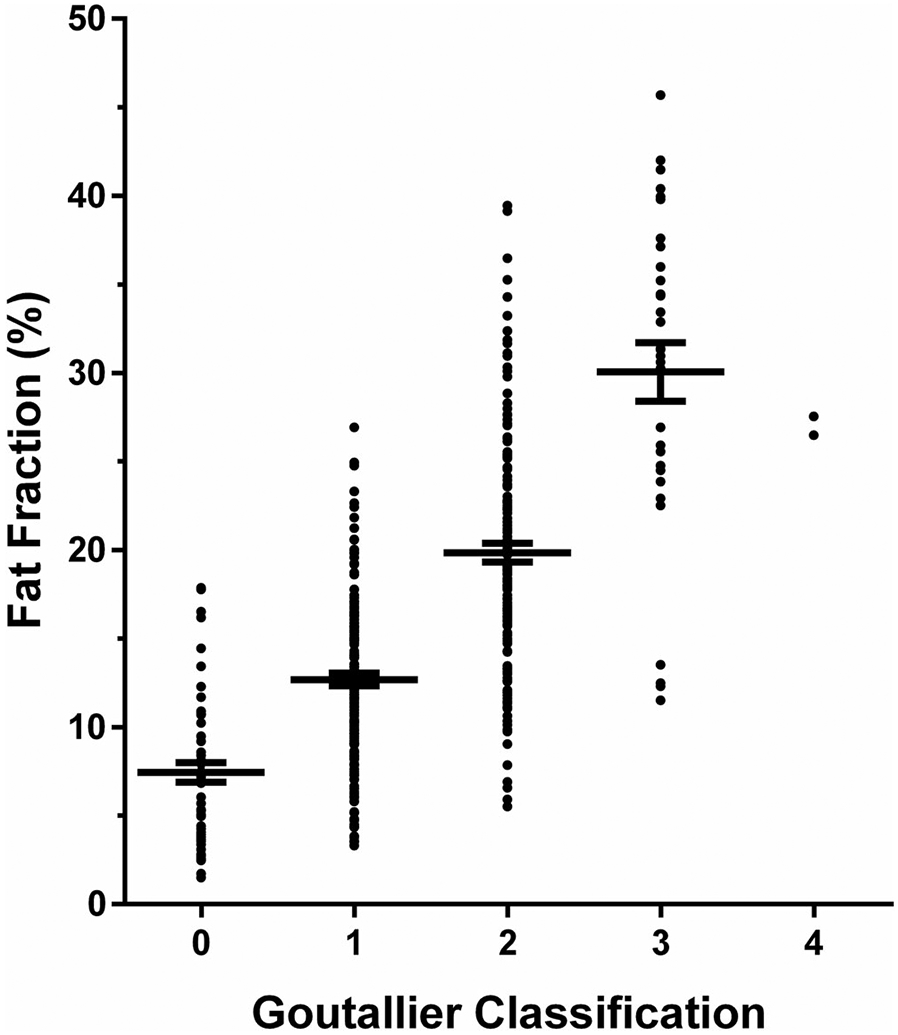
Results: The FF showed excellent intra- and interreader agreement (ICC range: 0.97-0.99) and was significantly associated with GC at all spinal levels. Subgroup analysis suggested that early/subtle changes in PSM are detectable with FF but not with GC, given the absence of significant associations between FF and GC (P-value range: 0.036 at L5/S1 to 0.784 at L2/L3). Averaged over all spinal levels, FF and GC were significantly associated with VAS scores.
Data conclusion: In the absence of FF, GC may be the best surrogate for PSM quality. Given the ability of CSE-MRI to detect muscle alterations at early stages of PSM degeneration, this technique may have potential for further investigations of the role of PSM in chronic LBP.
Level of evidence: 2 TECHNICAL EFFICACY STAGE: 2.
Keywords: Goutallier classification; chemical shift; fat fraction; low back pain; paraspinal musculature.
© 2022 The Authors. Journal of Magnetic Resonance Imaging published by Wiley Periodicals LLC on behalf of International Society for Magnetic Resonance in Medicine.
Conflict of interest statement
Conflict of Interest
The authors declare no conflict of interest.
Figures

Comment in
-
Editorial for "Paraspinal Muscle in Chronic Low Back Pain: Comparison Between Standard Parameters and Chemical Shift Encoding-Based Water-Fat MRI".J Magn Reson Imaging. 2022 Nov;56(5):1609-1610. doi: 10.1002/jmri.28144. Epub 2022 Mar 7. J Magn Reson Imaging. 2022. PMID: 35253949 No abstract available.
References
-
- Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet 2018;391(10137):2356–2367. - PubMed
-
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388(10053):1545–1602. - PMC - PubMed
-
- Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet 2017;389(10070):736–747. - PubMed
-
- Chou D, Samartzis D, Bellabarba C, et al. Degenerative magnetic resonance imaging changes in patients with chronic low back pain: A systematic review. Spine 2011;36(21 Suppl):S43–S53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
