

Phenotype-Directed Management of Hypertension in Pregnancy
- PMID: 35285667
- PMCID: PMC9075436
- DOI: 10.1161/JAHA.121.023694
Phenotype-Directed Management of Hypertension in Pregnancy
Abstract
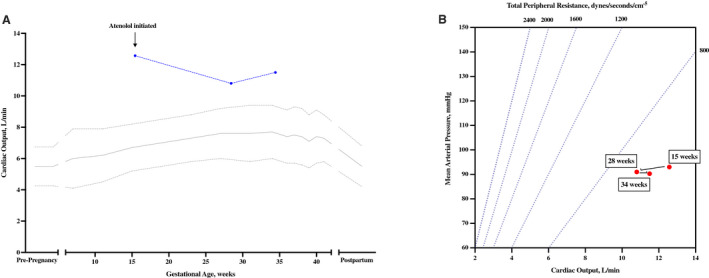
Hypertensive disorders of pregnancy are among the most serious conditions that pregnancy care providers face; however, little attention has been paid to the concept of tailoring clinical care to reduce associated adverse maternal and perinatal outcomes based on the underlying disease pathogenesis. This narrative review discusses the integration of phenotype-based clinical strategies in the management of high-risk pregnant patients that are currently not common clinical practice: real-time placental growth factor testing at Mount Sinai Hospital, Toronto and noninvasive hemodynamic monitoring to guide antihypertensive therapy at the University of Washington Medical Center, Seattle. Future work should focus on promoting more widespread integration of these novel strategies into obstetric care to improve outcomes of pregnancies at high risk of adverse maternal-fetal outcomes from these complications of pregnancy.
Keywords: antihypertensive agents; female sex; hemodynamic monitoring; humans; hypertension, pregnancy‐induced; placenta growth factor; pregnancy.
Figures





References
-
- Grandi SM, Filion KB, Yoon S, Ayele HT, Doyle CM, Hutcheon JA, Smith GN, Gore GC, Ray JG, Nerenberg K, et al. Cardiovascular disease‐related morbidity and mortality in women with a history of pregnancy complications. Circulation. 2019;139:1069–1079. doi: 10.1161/CIRCULATIONAHA.118.036748 - DOI - PubMed
-
- Leon LJ, McCarthy FP, Direk K, Gonzalez‐Izquierdo A, Prieto‐Merino D, Casas JP, Chappell L. Preeclampsia and cardiovascular disease in a large UK pregnancy cohort of linked electronic health records: a CALIBER study. Circulation. 2019;140:1050–1060. doi: 10.1161/CIRCULATIONAHA.118.038080 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
