

Per- and Polyfluoroalkyl Substances and Risk of Myocardial Infarction and Stroke: A Nested Case-Control Study in Sweden
- PMID: 35285690
- PMCID: PMC8919955
- DOI: 10.1289/EHP9791
Per- and Polyfluoroalkyl Substances and Risk of Myocardial Infarction and Stroke: A Nested Case-Control Study in Sweden
Abstract
Background: Per- and polyfluoroalkyl substances (PFAS) are widespread and persistent pollutants that have been associated with elevated cholesterol levels. However, data on incident cardiovascular disease (CVD) is lacking.
Objectives: We investigated the association of exposure to PFAS with risk of myocardial infarction and stroke and, subsidiary, with baseline blood lipids.
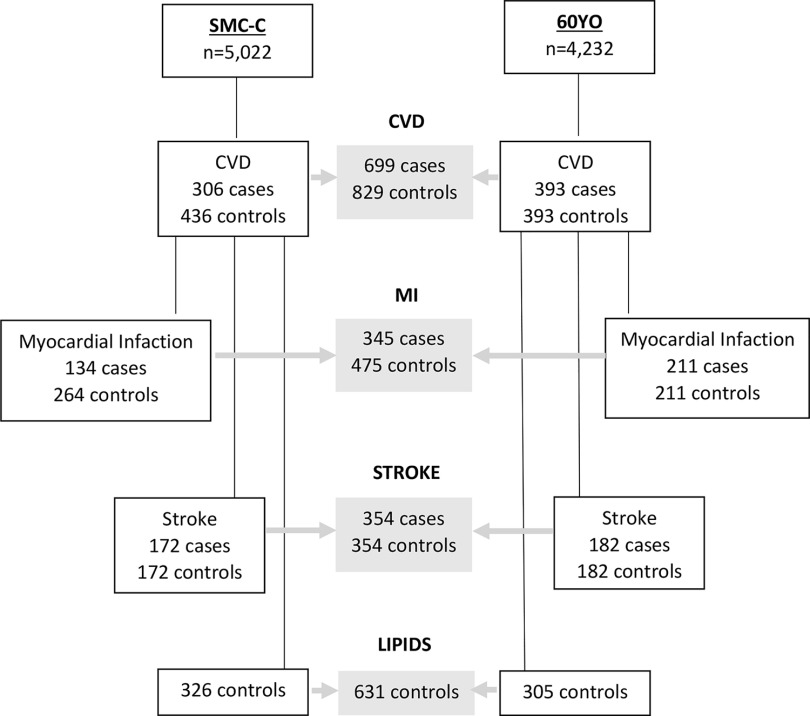
Methods: This population-based nested case-control study included first incident myocardial infarction and stroke cases with matched controls from two Swedish cohorts: the Swedish Mammography Cohort-Clinical (SMC-C) and the Cohort of 60-year-olds (60YO). Baseline blood sampling occurred during 2003-2009 and 1997-1999 with follow-up through 2017 and 2014 for the SMC-C and the 60YO, respectively. Eight plasma PFAS concentrations were measured using targeted liquid chromatography-triple quadrupole mass spectrometry. Five of these were quantifiable in both cohorts; individual values and their standardized sum were categorized into tertiles based on the controls. First incident myocardial infarction () and ischemic stroke () cases were ascertained via linkage to the National Inpatient Register and the Cause of Death Register. Controls were randomly selected from each cohort after matching for age, sex, and sample date. Baseline blood lipids were measured in plasma or serum after overnight fasting.
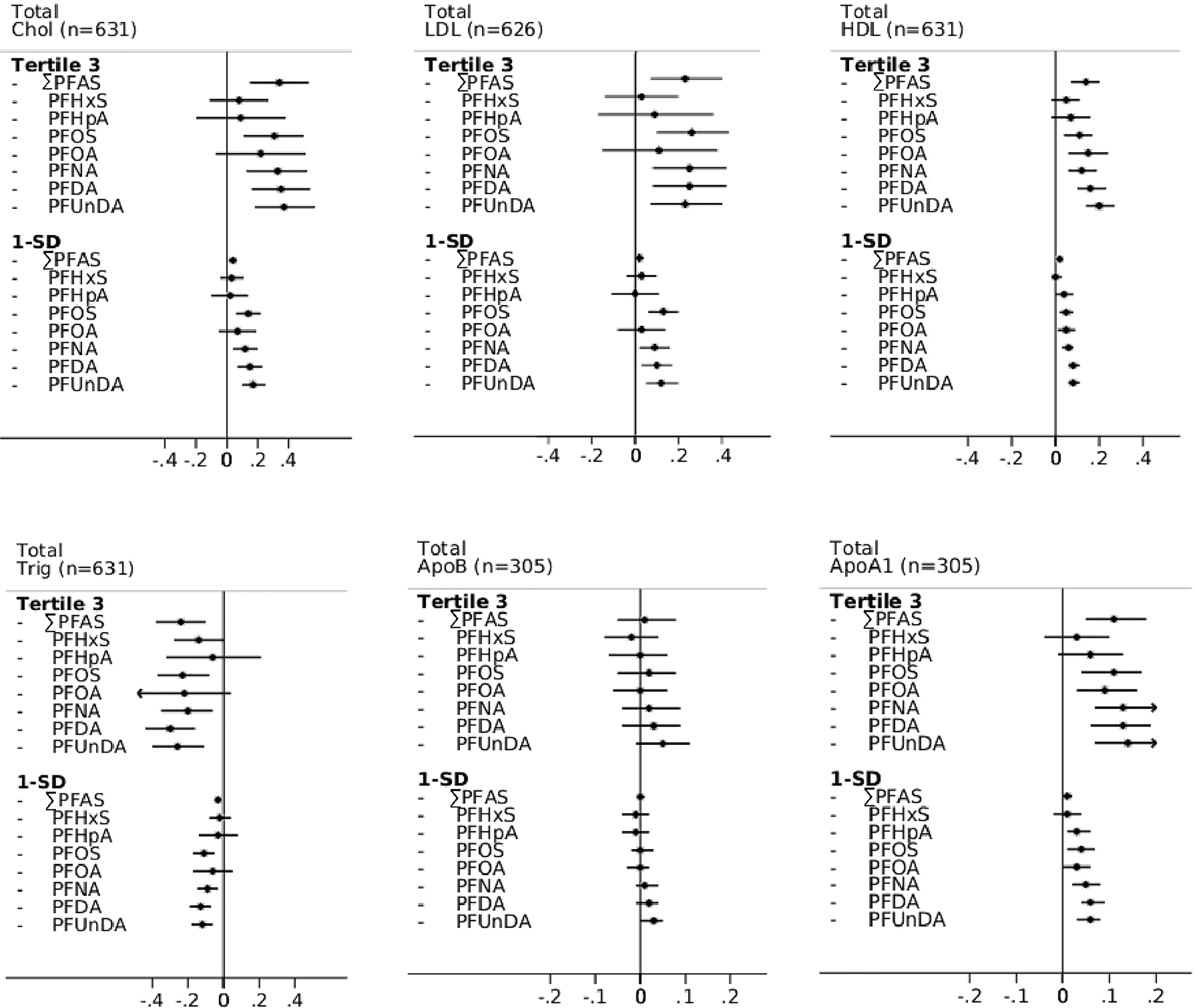
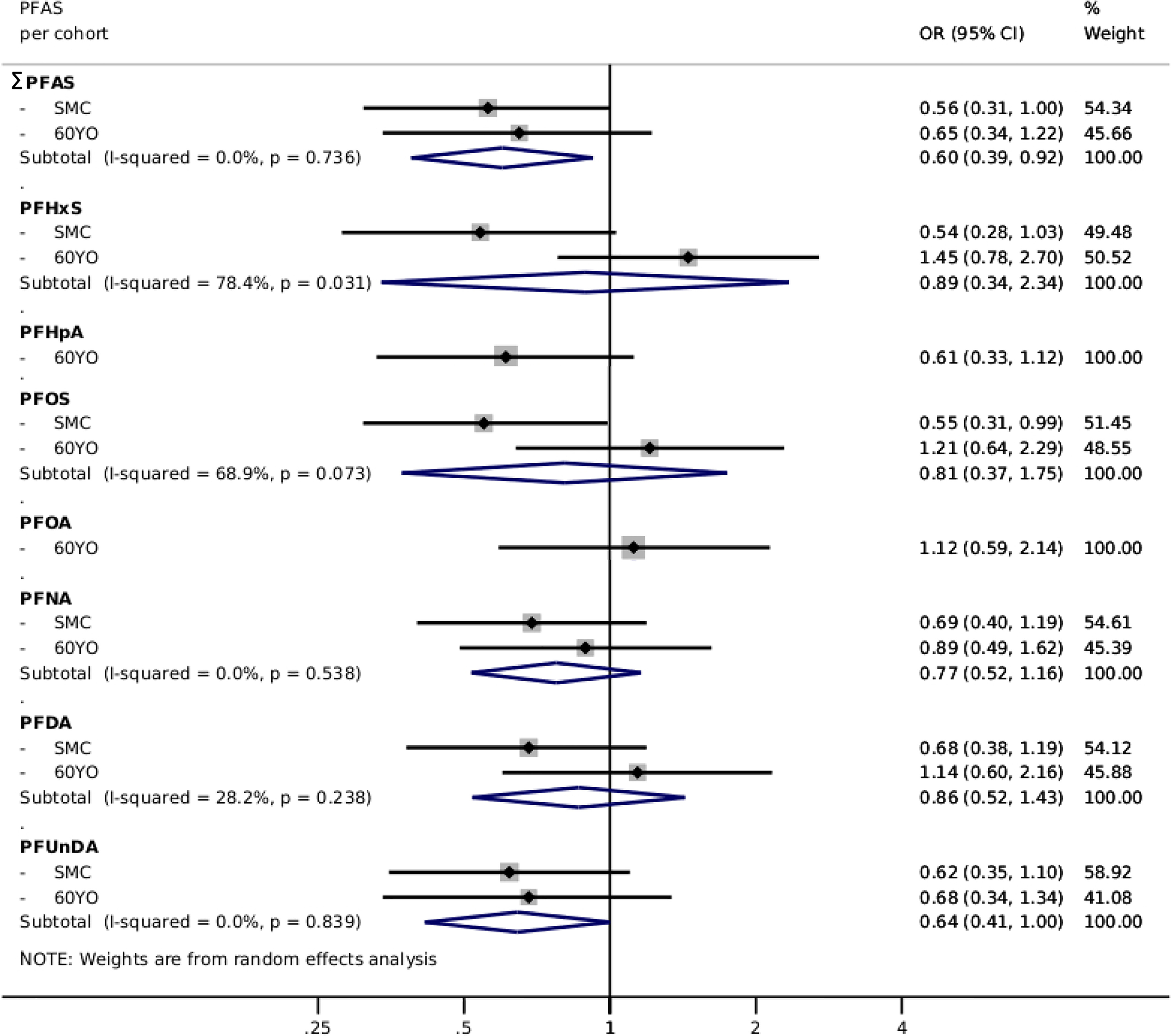
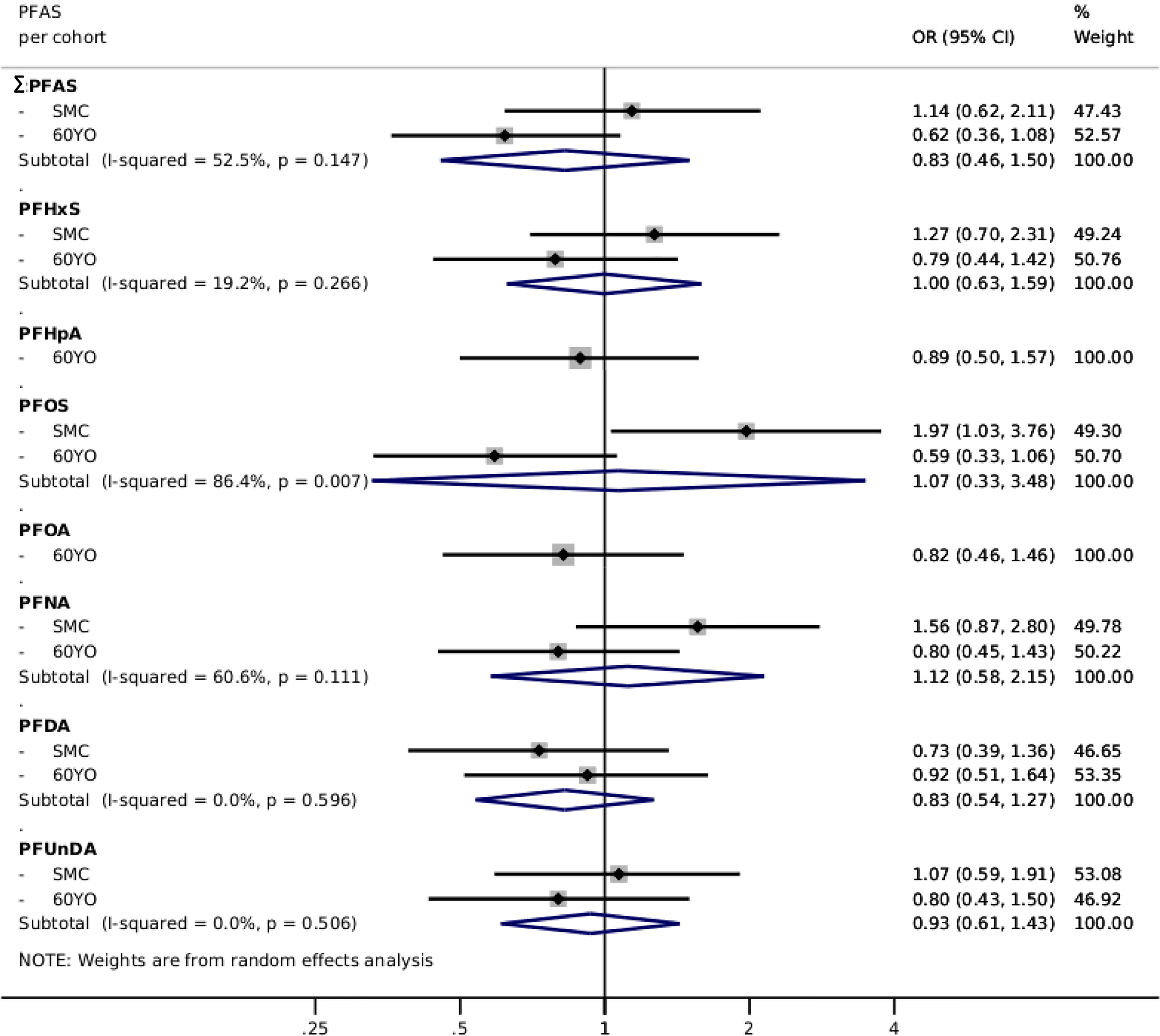
Results: Among the 1,528 case-control subjects, the mean (standard deviation) age was 66 (7.7) y and 67% of them were women. In multivariable-adjusted analyses, the third tertile of the standardized sum of five PFAS associated with higher cholesterol and lower triglyceride levels among controls at baseline (). The corresponding results were [95% confidence interval (CI): 0.53, 0.93] for CVD, 0.60 (95% CI: 0.39, 0.92) for myocardial infarction, and 0.83 (95% CI: 0.46, 1.50) for stroke.
Discussion: This study indicated that exposure to PFAS, although associated with increased cholesterol levels, did not associate with an increased risk of myocardial infarction, stroke, or their composite end point. The findings improve our knowledge on potential health effects of environmental contaminants in the CVD context. https://doi.org/10.1289/EHP9791.
Figures
References
-
- ATSDR (Agency for Toxic Substances and Disease Registry). 2021. Toxicological profile for perfluoroalkyls. Atlanta, GA: ATSDR. https://www.atsdr.cdc.gov/ToxProfiles/tp200.pdf [accessed 10 March 2022]. - PubMed
-
- Behr AC, Kwiatkowski A, Ståhlman M, Schmidt FF, Luckert C, Braeuning A, et al. 2020. Impairment of bile acid metabolism by perfluorooctanoic acid (PFOA) and perfluorooctanesulfonic acid (PFOS) in human HepaRG hepatoma cells. Arch Toxicol 94(5):1673–1686, PMID: , 10.1007/s00204-020-02732-3. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials