

Evaluating the Association Between Low-Density Lipoprotein Cholesterol Reduction and Relative and Absolute Effects of Statin Treatment: A Systematic Review and Meta-analysis
- PMID: 35285850
- PMCID: PMC8922205
- DOI: 10.1001/jamainternmed.2022.0134
Evaluating the Association Between Low-Density Lipoprotein Cholesterol Reduction and Relative and Absolute Effects of Statin Treatment: A Systematic Review and Meta-analysis
Erratum in
-
Error in Figure 3.JAMA Intern Med. 2022 May 1;182(5):579. doi: 10.1001/jamainternmed.2022.1671. JAMA Intern Med. 2022. PMID: 35499770 Free PMC article. No abstract available.
Abstract
Importance: The association between statin-induced reduction in low-density lipoprotein cholesterol (LDL-C) levels and the absolute risk reduction of individual, rather than composite, outcomes, such as all-cause mortality, myocardial infarction, or stroke, is unclear.
Objective: To assess the association between absolute reductions in LDL-C levels with treatment with statin therapy and all-cause mortality, myocardial infarction, and stroke to facilitate shared decision-making between clinicians and patients and inform clinical guidelines and policy.
Data sources: PubMed and Embase were searched to identify eligible trials from January 1987 to June 2021.
Study selection: Large randomized clinical trials that examined the effectiveness of statins in reducing total mortality and cardiovascular outcomes with a planned duration of 2 or more years and that reported absolute changes in LDL-C levels. Interventions were treatment with statins (3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors) vs placebo or usual care. Participants were men and women older than 18 years.
Data extraction and synthesis: Three independent reviewers extracted data and/or assessed the methodological quality and certainty of the evidence using the risk of bias 2 tool and Grading of Recommendations, Assessment, Development and Evaluation. Any differences in opinion were resolved by consensus. Meta-analyses and a meta-regression were undertaken.
Main outcomes and measures: Primary outcome: all-cause mortality. Secondary outcomes: myocardial infarction, stroke.
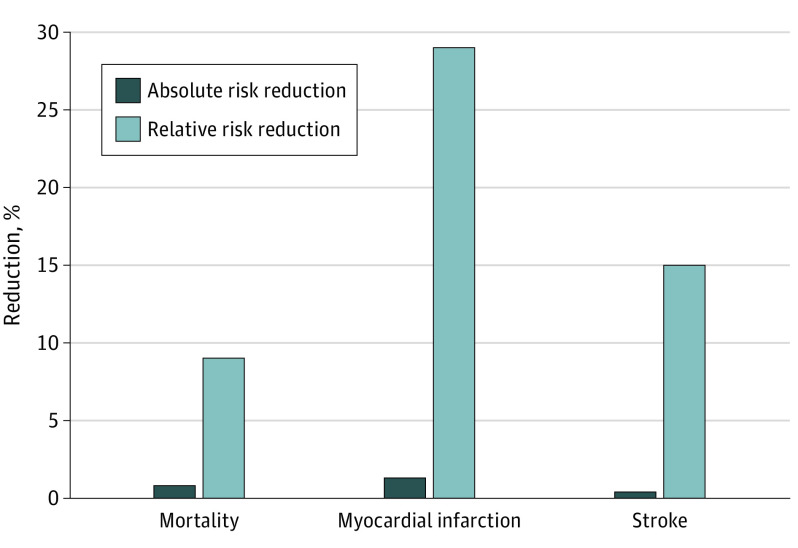
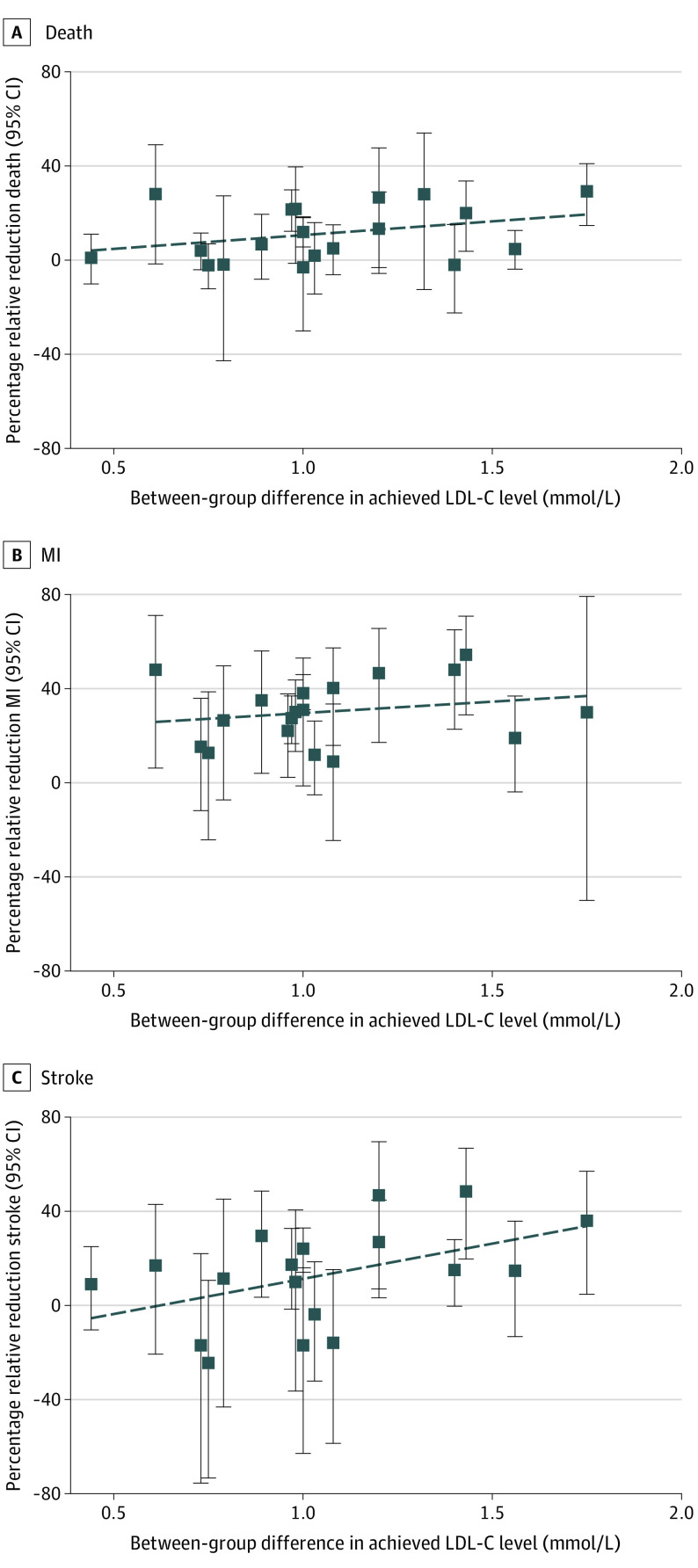
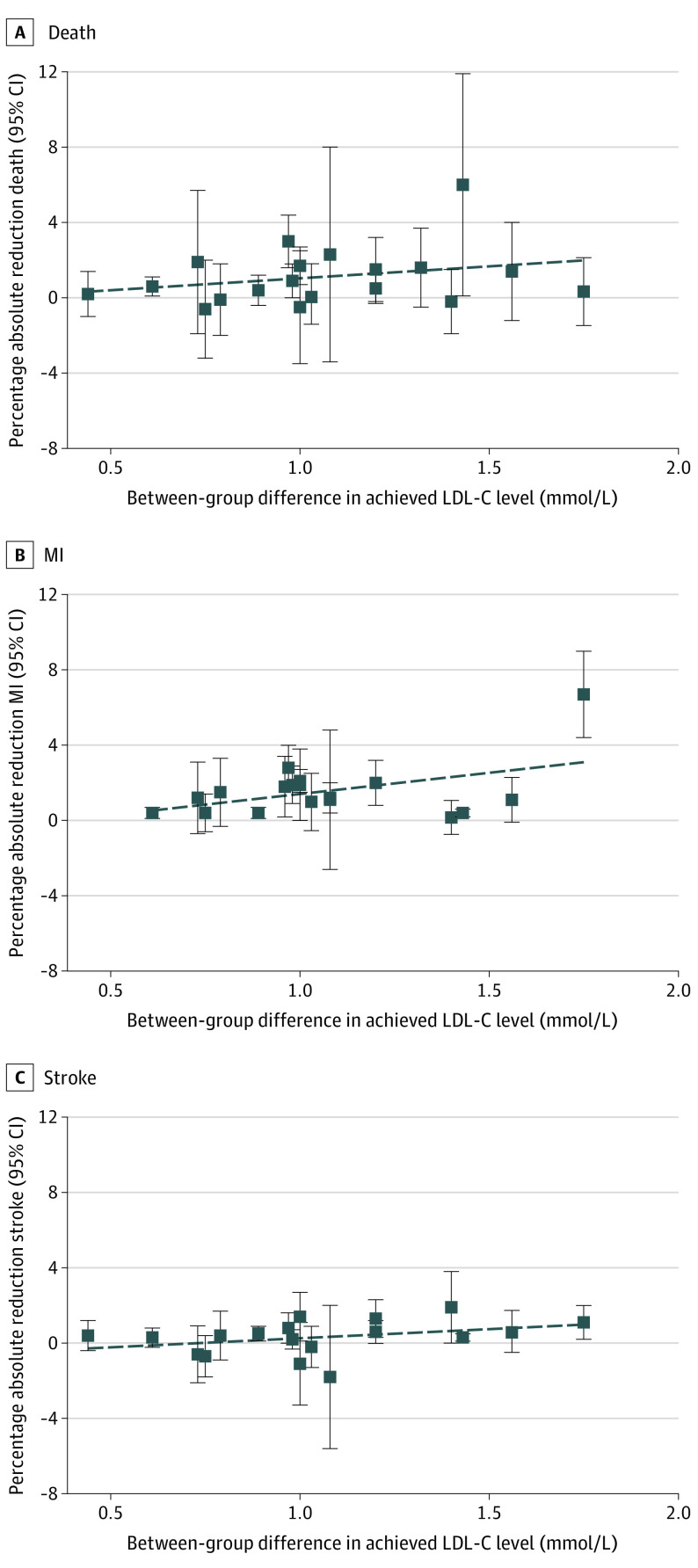
Findings: Twenty-one trials were included in the analysis. Meta-analyses showed reductions in the absolute risk of 0.8% (95% CI, 0.4%-1.2%) for all-cause mortality, 1.3% (95% CI, 0.9%-1.7%) for myocardial infarction, and 0.4% (95% CI, 0.2%-0.6%) for stroke in those randomized to treatment with statins, with associated relative risk reductions of 9% (95% CI, 5%-14%), 29% (95% CI, 22%-34%), and 14% (95% CI, 5%-22%) respectively. A meta-regression exploring the potential mediating association of the magnitude of statin-induced LDL-C reduction with outcomes was inconclusive.
Conclusions and relevance: The results of this meta-analysis suggest that the absolute risk reductions of treatment with statins in terms of all-cause mortality, myocardial infarction, and stroke are modest compared with the relative risk reductions, and the presence of significant heterogeneity reduces the certainty of the evidence. A conclusive association between absolute reductions in LDL-C levels and individual clinical outcomes was not established, and these findings underscore the importance of discussing absolute risk reductions when making informed clinical decisions with individual patients.
Conflict of interest statement
Figures
Comment in
-
Emphasizing Study Selection in a Review of Statin Treatment Effects and Low-Density Lipoprotein Cholesterol-Reply.JAMA Intern Med. 2022 Aug 1;182(8):891. doi: 10.1001/jamainternmed.2022.2217. JAMA Intern Med. 2022. PMID: 35759256 No abstract available.
-
Emphasizing Study Selection in a Review of Statin Treatment Effects and Low-Density Lipoprotein Cholesterol.JAMA Intern Med. 2022 Aug 1;182(8):890-891. doi: 10.1001/jamainternmed.2022.2214. JAMA Intern Med. 2022. PMID: 35759275 No abstract available.
References
-
- Grundy SM, Stone NJ, Bailey AL, et al. . 2018 AHA/ACC/AACVPR/ AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. - PMC - PubMed
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults . Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA. 2001;285(19):2486-2497. doi:10.1001/jama.285.19.2486 - DOI - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. ; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 pt B):2889-2934. doi:10.1016/j.jacc.2013.11.002 - DOI - PubMed
-
- Baigent C, Blackwell L, Emberson J, et al. ; Cholesterol Treatment Trialists’ Collaboration . Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. doi:10.1016/S0140-6736(10)61350-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
