

Factors Associated With Penicillin Allergy Labels in Electronic Health Records of Children in 2 Large US Pediatric Primary Care Networks
- PMID: 35285918
- PMCID: PMC9907342
- DOI: 10.1001/jamanetworkopen.2022.2117
Factors Associated With Penicillin Allergy Labels in Electronic Health Records of Children in 2 Large US Pediatric Primary Care Networks
Abstract
Importance: Penicillin allergy labels influence clinical decision-making, yet most children who are labeled do not have type 1 hypersensitivity allergic reactions and instead have a history of predictable adverse reactions or unspecified illness symptoms while receiving penicillin for viral infections. Studies describing penicillin allergy labeling in the pediatric outpatient setting are lacking.
Objective: To describe the epidemiology and factors associated with penicillin allergy labels across 2 large US pediatric primary care networks.
Design, setting, and participants: This retrospective, longitudinal birth cohort study was conducted in 90 primary care pediatric practices serving a diverse population of children across Houston, Texas, Austin, Texas, Philadelphia, Pennsylvania, and parts of New Jersey. Participants were children born between January 2010 and June 2020 who had a health care visit in the first 14 days of life and at least 2 additional visits in the first year of life at one of 90 primary care pediatric practices. Censoring criteria were additionally applied to exclude data from children no longer seeking health care in the 90 clinics over time. Statistical analysis was performed from February to May 2021.
Exposures: Basic patient demographics, health care utilization, penicillin exposure, and primary clinic location.
Main outcomes and measures: Addition of penicillin allergy label in the electronic medical record.
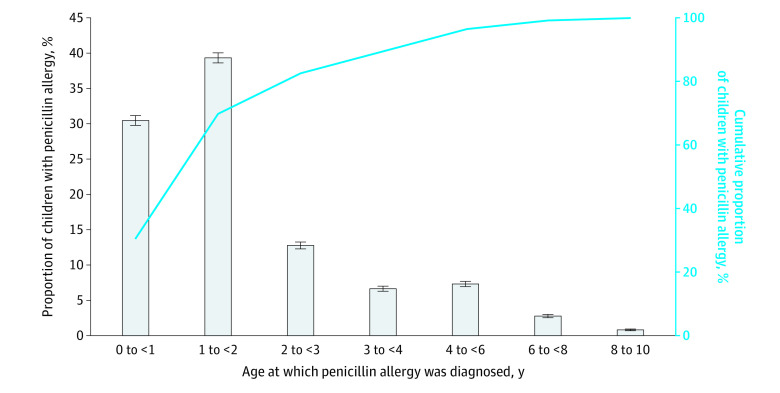
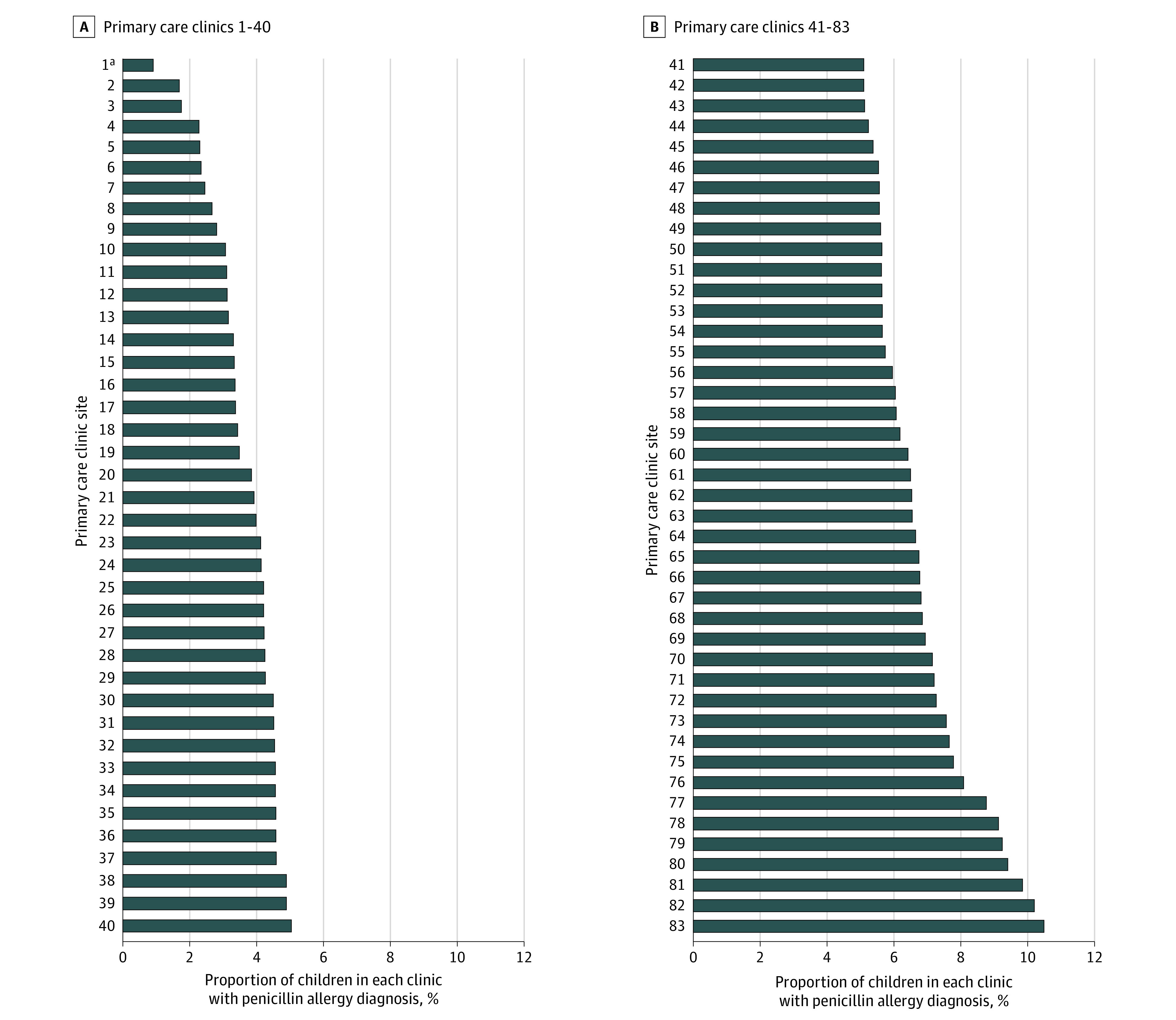
Results: Among 334 465 children in the birth cohort, 164 173 (49.1%) were female; 72 831 (21.8%) were Hispanic, 59 598 (17.8%) were non-Hispanic Black, and 148 534 (44.4%) were non-Hispanic White; the median (IQR) age at censoring was 3.8 (1.7-6.6) years; 18 015 (5.4%) were labeled as penicillin allergic, but the prevalence of penicillin allergy labeling ranged from 0.9% to 10.2% across practices. Children were labeled at a median (IQR) age of 1.3 (0.9-2.3) years. Non-Hispanic White children were more likely to be labeled compared with non-Hispanic Black children after controlling for potential confounders (adjusted odds ratio, 1.7 [95% CI, 1.6-1.8]). There were 6797 allergic children (37.7%) labeled after receiving 1 penicillin prescription and 1423 (7.9%) labeled after receiving 0 penicillin prescriptions.
Conclusions and relevance: In this cohort study of more than 330 000 children, penicillin allergy labeling was common and varied widely across practices. Children were labeled early in life, and almost half were labeled after receiving 1 or 0 penicillin prescriptions. These findings raise questions regarding the validity of penicillin allergy labels. Future work exploring the fidelity of and outcomes associated with penicillin allergy-labeling in children is warranted.
Conflict of interest statement
Figures
References
-
- Kerr JR. Penicillin allergy: a study of incidence as reported by patients. Br J Clin Pract. 1994;48(1):5-7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
