

Effect of Internet-Based vs Face-to-Face Cognitive Behavioral Therapy for Adults With Obsessive-Compulsive Disorder: A Randomized Clinical Trial
- PMID: 35285923
- PMCID: PMC9907343
- DOI: 10.1001/jamanetworkopen.2022.1967
Effect of Internet-Based vs Face-to-Face Cognitive Behavioral Therapy for Adults With Obsessive-Compulsive Disorder: A Randomized Clinical Trial
Erratum in
-
Error in Figure 2B.JAMA Netw Open. 2022 Jul 1;5(7):e2222742. doi: 10.1001/jamanetworkopen.2022.22742. JAMA Netw Open. 2022. PMID: 35796215 Free PMC article. No abstract available.
-
Error in Results.JAMA Netw Open. 2023 Jun 1;6(6):e2323948. doi: 10.1001/jamanetworkopen.2023.23948. JAMA Netw Open. 2023. PMID: 37389882 Free PMC article. No abstract available.
Abstract
Importance: Cognitive behavioral therapy (CBT) for obsessive-compulsive disorder (OCD) is a highly specialized treatment that is in short supply worldwide.
Objectives: To investigate whether both therapist-guided and unguided internet-based CBT (ICBT) are noninferior to face-to-face CBT for adults with OCD, to conduct a health economic evaluation, and to determine whether treatment effects were moderated by source of participant referral.
Design, setting, and participants: This study is a single-blinded, noninferiority, randomized clinical trial, with a full health economic evaluation, conducted between September 2015 and January 2020, comparing therapist-guided ICBT, unguided ICBT, and individual face-to-face CBT for adults with OCD. Follow-up data were collected up to 12 months after treatment. The study was conducted at 2 specialist outpatient OCD clinics in Stockholm, Sweden. Participants included a consecutive sample of adults with a primary diagnosis of OCD, either self-referred or referred by a clinician. Data analysis was performed from June 2019 to January 2022.
Interventions: Guided ICBT, unguided ICBT, and face-to-face CBT delivered over 14 weeks.
Main outcomes and measures: The primary end point was the change in OCD symptom severity from baseline to 3-month follow-up. The noninferiority margin was 3 points on the masked assessor-rated Yale-Brown Obsessive Compulsive Scale.
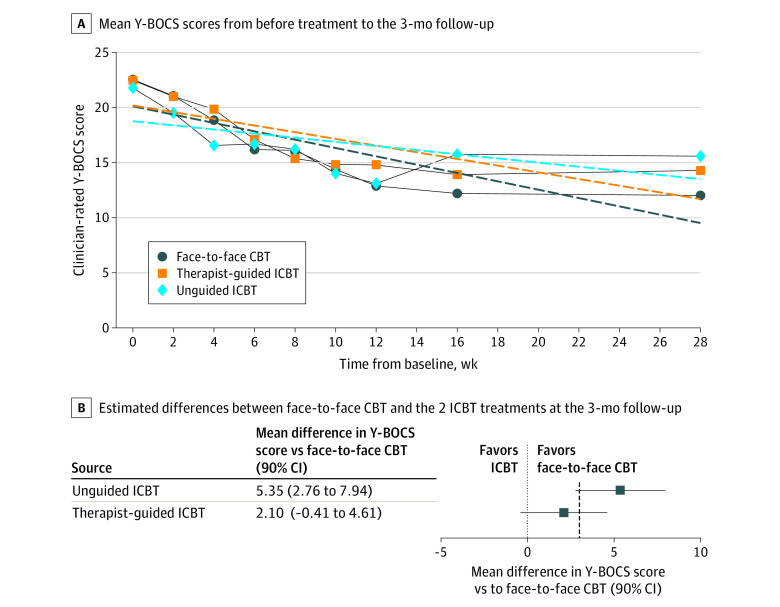
Results: A total of 120 participants were enrolled (80 women [67%]; mean [SD] age, 32.24 [9.64] years); 38 were randomized to the face-to-face CBT group, 42 were randomized to the guided ICBT group, and 40 were randomized to the unguided ICBT group. The mean difference between therapist-guided ICBT and face-to-face CBT at the primary end point was 2.10 points on the Yale-Brown Obsessive Compulsive Scale (90% CI, -0.41 to 4.61 points; P = .17), favoring face-to-face CBT, meaning that the primary noninferiority results were inconclusive. The difference between unguided ICBT and face-to-face CBT was 5.35 points (90% CI, 2.76 to 7.94 points; P < .001), favoring face-to-face CBT. The health economic analysis showed that both guided and unguided ICBT were cost-effective compared with face-to-face CBT. Source of referral did not moderate treatment outcome. The most common adverse events were anxiety (30 participants [25%]), depressive symptoms (20 participants [17%]), and stress (11 participants [9%]).
Conclusions and relevance: The findings of this randomized clinical trial of ICBT vs face-to-face CBT for adults with OCD do not conclusively demonstrate noninferiority. Therapist-guided ICBT could be a cost-effective alternative to in-clinic CBT for adults with OCD in scenarios where traditional CBT is not readily available; unguided ICBT is probably less efficacious but could be an alternative when providing remote clinician support is not feasible.
Trial registration: ClinicalTrials.gov Identifier: NCT02541968.
Conflict of interest statement
Figures


Comment in
-
Focusing on Accessibility of Evidence-Based Treatments for Obsessive-Compulsive Disorder.JAMA Netw Open. 2022 Mar 1;5(3):e221978. doi: 10.1001/jamanetworkopen.2022.1978. JAMA Netw Open. 2022. PMID: 35285927 Free PMC article. No abstract available.
Similar articles
-
Study protocol for a single-blind, randomised controlled, non-inferiority trial of internet-based versus face-to-face cognitive behaviour therapy for obsessive-compulsive disorder.BMJ Open. 2018 Sep 5;8(9):e022254. doi: 10.1136/bmjopen-2018-022254. BMJ Open. 2018. PMID: 30185575 Free PMC article.
-
Therapist-Assisted Internet-Based Cognitive Behavioral Therapy Versus Progressive Relaxation in Obsessive-Compulsive Disorder: Randomized Controlled Trial.J Med Internet Res. 2018 Aug 8;20(8):e242. doi: 10.2196/jmir.9566. J Med Internet Res. 2018. PMID: 30089607 Free PMC article. Clinical Trial.
-
Effect of an Internet-Delivered Stepped-Care Program vs In-Person Cognitive Behavioral Therapy on Obsessive-Compulsive Disorder Symptoms in Children and Adolescents: A Randomized Clinical Trial.JAMA. 2021 May 11;325(18):1863-1873. doi: 10.1001/jama.2021.3839. JAMA. 2021. PMID: 33974020 Free PMC article. Clinical Trial.
-
Internet-Delivered Cognitive Behavioural Therapy for Post-traumatic Stress Disorder or Acute Stress Disorder: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Jun 1;21(9):1-120. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34527087 Free PMC article.
-
Acceptability, feasibility, and efficacy of Internet cognitive behavioral therapy (iCBT) for pediatric obsessive-compulsive disorder: a systematic review.Syst Rev. 2019 Nov 20;8(1):284. doi: 10.1186/s13643-019-1166-6. Syst Rev. 2019. PMID: 31747935 Free PMC article.
Cited by
-
Longitudinal study of gut microbiome in obsessive-compulsive disorder.Brain Behav. 2023 Aug;13(8):e3115. doi: 10.1002/brb3.3115. Epub 2023 Jun 5. Brain Behav. 2023. PMID: 37277984 Free PMC article.
-
Examining Change in the Frequency of Adaptive Actions as a Mediator of Treatment Outcomes in Internet-Delivered Therapy for Depression and Anxiety.J Clin Med. 2022 Oct 11;11(20):6001. doi: 10.3390/jcm11206001. J Clin Med. 2022. PMID: 36294322 Free PMC article.
-
Cost-effectiveness of internet-delivered cognitive behaviour therapy for body dysmorphic disorder: Results from a randomised controlled trial.Internet Interv. 2023 Jan 24;31:100604. doi: 10.1016/j.invent.2023.100604. eCollection 2023 Mar. Internet Interv. 2023. PMID: 36756354 Free PMC article.
-
Error in Figure 2B.JAMA Netw Open. 2022 Jul 1;5(7):e2222742. doi: 10.1001/jamanetworkopen.2022.22742. JAMA Netw Open. 2022. PMID: 35796215 Free PMC article. No abstract available.
-
Therapist-supported Internet-based cognitive behaviour therapy yields similar effects as face-to-face therapy for psychiatric and somatic disorders: an updated systematic review and meta-analysis.World Psychiatry. 2023 Jun;22(2):305-314. doi: 10.1002/wps.21088. World Psychiatry. 2023. PMID: 37159350 Free PMC article.
References
-
- National Collaborating Centre for Mental Health (UK) . Obsessive-compulsive disorder: core interventions in the treatment of obsessive-compulsive disorder and body dysmorphic disorder. British Psychological Society; 2006. Accessed September 30, 2021. https://www.ncbi.nlm.nih.gov/books/NBK56458/ - PubMed
-
- Andersson E, Hedman E, Enander J, et al. . D-cycloserine vs placebo as adjunct to cognitive behavioral therapy for obsessive-compulsive disorder and interaction with antidepressants: a randomized clinical trial. JAMA Psychiatry. 2015;72(7):659-667. doi:10.1001/jamapsychiatry.2015.0546 - DOI - PubMed
