

The impact of surgical delay on resectability of colorectal cancer: An international prospective cohort study
- PMID: 35286766
- PMCID: PMC9322431
- DOI: 10.1111/codi.16117
The impact of surgical delay on resectability of colorectal cancer: An international prospective cohort study
Abstract
Aim: The SARS-CoV-2 pandemic has provided a unique opportunity to explore the impact of surgical delays on cancer resectability. This study aimed to compare resectability for colorectal cancer patients undergoing delayed versus non-delayed surgery.
Methods: This was an international prospective cohort study of consecutive colorectal cancer patients with a decision for curative surgery (January-April 2020). Surgical delay was defined as an operation taking place more than 4 weeks after treatment decision, in a patient who did not receive neoadjuvant therapy. A subgroup analysis explored the effects of delay in elective patients only. The impact of longer delays was explored in a sensitivity analysis. The primary outcome was complete resection, defined as curative resection with an R0 margin.
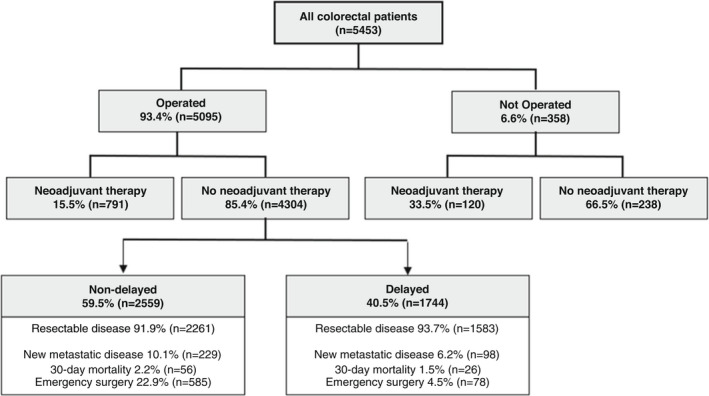
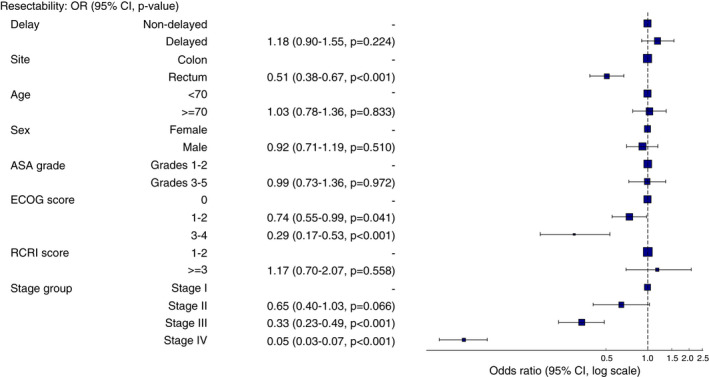
Results: Overall, 5453 patients from 304 hospitals in 47 countries were included, of whom 6.6% (358/5453) did not receive their planned operation. Of the 4304 operated patients without neoadjuvant therapy, 40.5% (1744/4304) were delayed beyond 4 weeks. Delayed patients were more likely to be older, men, more comorbid, have higher body mass index and have rectal cancer and early stage disease. Delayed patients had higher unadjusted rates of complete resection (93.7% vs. 91.9%, P = 0.032) and lower rates of emergency surgery (4.5% vs. 22.5%, P < 0.001). After adjustment, delay was not associated with a lower rate of complete resection (OR 1.18, 95% CI 0.90-1.55, P = 0.224), which was consistent in elective patients only (OR 0.94, 95% CI 0.69-1.27, P = 0.672). Longer delays were not associated with poorer outcomes.
Conclusion: One in 15 colorectal cancer patients did not receive their planned operation during the first wave of COVID-19. Surgical delay did not appear to compromise resectability, raising the hypothesis that any reduction in long-term survival attributable to delays is likely to be due to micro-metastatic disease.
Keywords: COVID-19; SARS-CoV-2; colorectal cancer; coronavirus; surgery; surgical delay.
© 2022 The Authors. Colorectal Disease published by John Wiley & Sons Ltd on behalf of Association of Coloproctology of Great Britain and Ireland.
Conflict of interest statement
There are no conflicts of interest to declare.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
