

Efficacy and safety of CD24Fc in hospitalised patients with COVID-19: a randomised, double-blind, placebo-controlled, phase 3 study
- PMID: 35286843
- PMCID: PMC8916779
- DOI: 10.1016/S1473-3099(22)00058-5
Efficacy and safety of CD24Fc in hospitalised patients with COVID-19: a randomised, double-blind, placebo-controlled, phase 3 study
Abstract
Background: Non-antiviral therapeutic options are required for the treatment of hospitalised patients with COVID-19. CD24Fc is an immunomodulator with potential to reduce the exaggerated inflammatory response to tissue injuries. We aimed to evaluate the safety and efficacy of CD24Fc in hospitalised adults with COVID-19 receiving oxygen support.
Methods: We conducted a randomised, double-blind, placebo-controlled, phase 3 study at nine medical centres in the USA. Hospitalised patients (age ≥18 years) with confirmed SARS-CoV-2 infection who were receiving oxygen support and standard of care were randomly assigned (1:1) by site-stratified block randomisation to receive a single intravenous infusion of CD24Fc 480 mg or placebo. The study funder, investigators, and patients were masked to treatment group assignment. The primary endpoint was time to clinical improvement over 28 days, defined as time that elapsed between a baseline National Institute of Allergy and Infectious Diseases ordinal scale score of 2-4 and reaching a score of 5 or higher or hospital discharge. The prespecified primary interim analysis was done when 146 participants reached the time to clinical improvement endpoint. Efficacy was assessed in the intention-to-treat population. Safety was assessed in the as-treated population. This study is registered with ClinicalTrials.gov, NCT04317040.
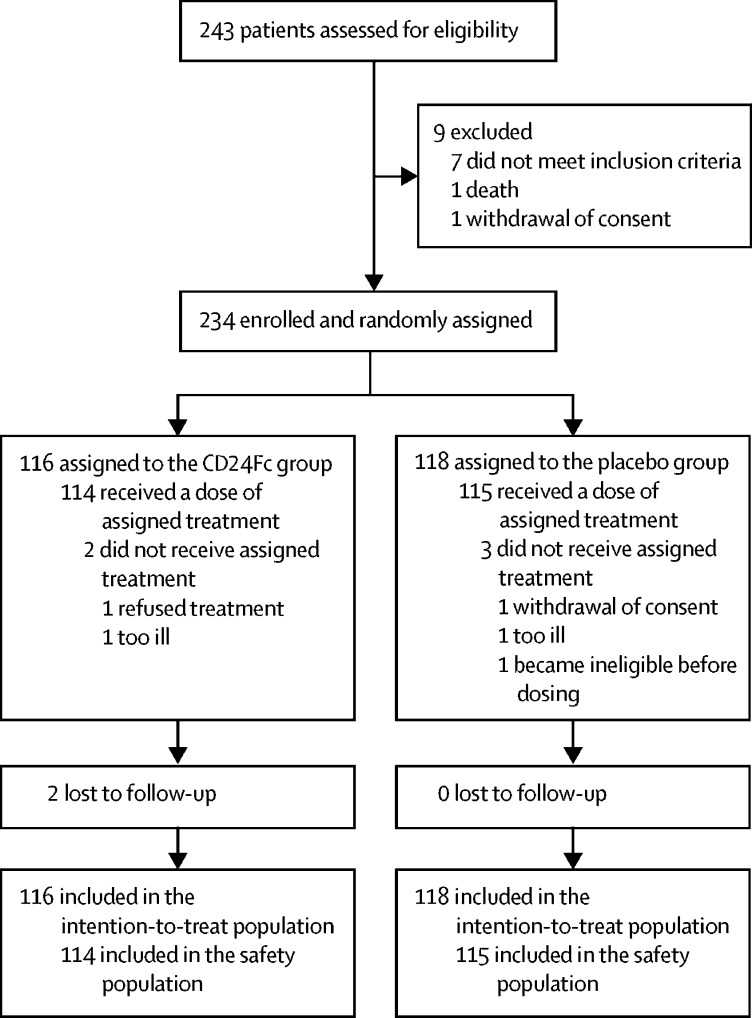
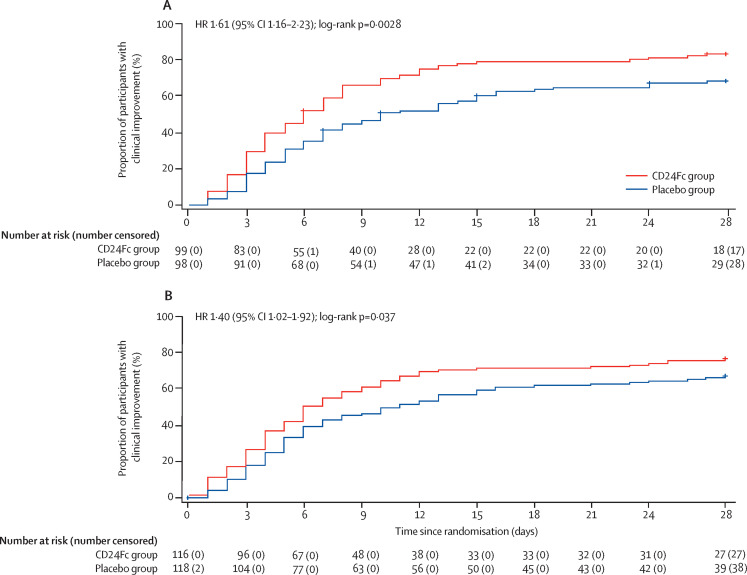
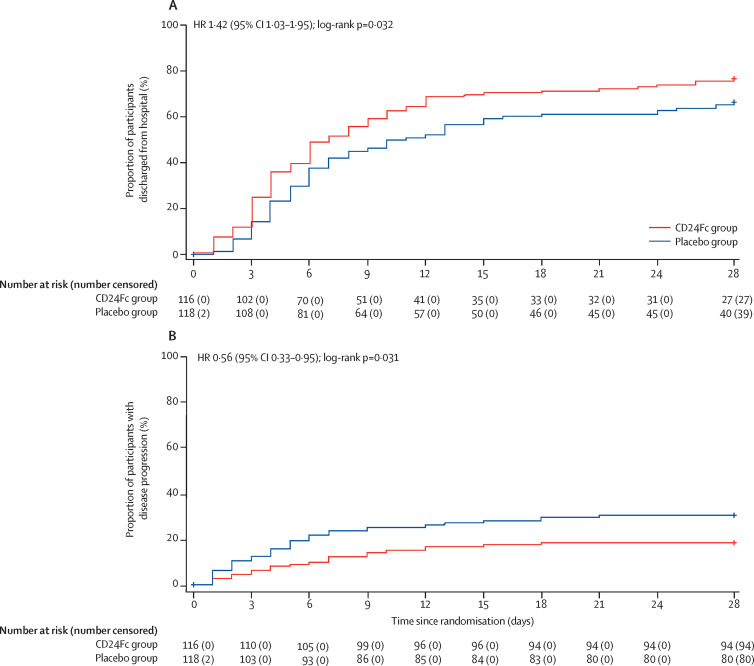
Findings: Between April 24 and Sept 22, 2020, 243 hospitalised patients were assessed for eligibility and 234 were enrolled and randomly assigned to receive CD24Fc (n=116) or placebo (n=118). The prespecified interim analysis was done when 146 participants reached the time to clinical improvement endpoint among 197 randomised participants. In the interim analysis, the 28-day clinical improvement rate was 82% (81 of 99) for CD24Fc versus 66% (65 of 98) for placebo; median time to clinical improvement was 6·0 days (95% CI 5·0-8·0) in the CD24Fc group versus 10·0 days (7·0-15·0) in the placebo group (hazard ratio [HR] 1·61, 95% CI 1·16-2·23; log-rank p=0·0028, which crossed the prespecified efficacy boundary [α=0·0147]). 37 participants were randomly assigned after the interim analysis data cutoff date; among the 234 randomised participants, median time to clinical improvement was 6·0 days (95% CI 5·0-9·0) in the CD24Fc group versus 10·5 days (7·0-15·0) in the placebo group (HR 1·40, 95% CI 1·02-1·92; log-rank p=0·037). The proportion of participants with disease progression within 28 days was 19% (22 of 116) in the CD24Fc group versus 31% (36 of 118) in the placebo group (HR 0·56, 95% CI 0·33-0·95; unadjusted p=0·031). The incidences of adverse events and serious adverse events were similar in both groups. No treatment-related adverse events were observed.
Interpretation: CD24Fc is generally well tolerated and accelerates clinical improvement of hospitalised patients with COVID-19 who are receiving oxygen support. These data suggest that targeting inflammation in response to tissue injuries might provide a therapeutic option for patients hospitalised with COVID-19.
Funding: Merck & Co, National Cancer Institute, OncoImmune.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests JW, JDP, ATC, CDM, EDW, DB, OKG, JEL, and SK had clinical trial agreements with OncoImmune. JDP reports payment for Baptist Medical Health COVID update (CME event). EDW was on the speaker's bureau at Merck & Co (before Merck's acquisition of OncoImmune). JEL is a consultant to Merck & Co for HIV-related studies. SK reports a grant from OncoImmune, during the conduct of the study; and grants from Merck & Co, Gilead Sciences, and Arbutus Pharmaceuticals, outside of the submitted work. ZL serves as a scientific advisory board member for Alphamab, Hengenix, and Ikonisys; and receives grants from Heat Biologics, National Institutes of Health, and Pelotonia, outside of the submitted work. EL, JiC, and XZ are employees of Edetek, the clinical data management and biostats service provider for OncoImmune. DB, DG, and AK are employees of Merck Sharp & Dohme, a subsidiary of Merck & Co, and could hold stocks or stock options in Merck & Co. H-YC, MD, RT, YL, and PZ are employees of OncoImmune, and received grants from National Institutes of Health and National Cancer Institute (R44CA246991-02S1), during the conduct of the study. MD, YL, and PZ have a patent or a patent pending. All other authors declare no competing interests.
Figures
Comment in
-
CD24Fc: an emerging COVID-19 therapy.Lancet Infect Dis. 2022 May;22(5):565-567. doi: 10.1016/S1473-3099(22)00125-6. Epub 2022 Mar 11. Lancet Infect Dis. 2022. PMID: 35286842 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
