

Antibiotic resistance among bacteria isolated from war-wounded patients at the Weapon Traumatology Training Center of the International Committee of the Red Cross from 2016 to 2019: a secondary analysis of WHONET surveillance data
- PMID: 35287597
- PMCID: PMC8922823
- DOI: 10.1186/s12879-022-07253-1
Antibiotic resistance among bacteria isolated from war-wounded patients at the Weapon Traumatology Training Center of the International Committee of the Red Cross from 2016 to 2019: a secondary analysis of WHONET surveillance data
Abstract
Background: A substantial body of evidence has recently emphasized the risks associated with antibiotic resistance (ABR) in conflicts in the Middle East. War-related, and more specifically weapon-related wounds can be an important breeding ground for multidrug resistant (MDR) organisms. However, the majority of available evidence comes from the military literature focused on risks and patterns of ABR in infections from combat-related injuries among military personnel. The overall aim of this study is to contribute to the scarce existing evidence on the burden of ABR among patients, including civilians with war-related wounds in the Middle East, in order to help inform the revision of empirical antibiotic prophylaxis and treatment protocols adopted in these settings. The primary objectives of this study are to: 1) describe the microbiology and the corresponding resistance profiles of the clinically relevant bacteria most commonly isolated from skin, soft tissue and bone biopsies in patients admitted to the WTTC; and 2) describe the association of the identified bacteria and corresponding resistance profiles with sociodemographic and specimen characteristics.
Methods: We retrospectively evaluated the antibiograms of all consecutive, non-duplicate isolates from samples taken from patients admitted to the ICRC WTTC between 2016 and 2019, limited to skin and soft tissue samples and bone biopsies. We collected data on socio-demographic characteristics from patient files and data on specimens from the WHONET database. We ran univariate and multivariable logistic regression models to test the association between bacterial and resistance profiles with sociodemographic and specimen characteristics.
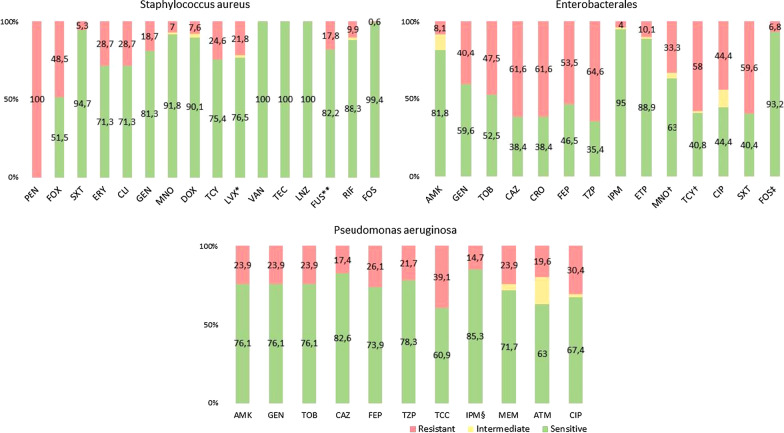
Results: Patients who were admitted with war-related trauma to the ICRC reconstructive surgical project in Tripoli, Lebanon, from 2016 to 2019, presented with high proportion of MDR in the samples taken from skin and soft tissues and bones, particularly Enterobacterales (44.6%), MRSA (44.6%) and P. aeruginosa (7.6%). The multivariable analysis shows that the odds of MDR isolates were higher in Iraqi patients (compared to Syrian patients) and in Enterobacterales isolates (compared to S. aureus isolates).
Conclusions: Our findings stress the importance of regularly screening patients who present with complex war-related injuries for colonization with MDR bacteria, and of ensuring an antibiotic-sensitivity testing-guided antimicrobial therapeutic approach.
Keywords: Bacterial drug resistance; Multidrug-resistance; Refugees; Vulnerable populations; War wounds; Wound infection.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. Antibiotic resistance - Fact sheets [Internet]. Antibiotic resistance. 2020. https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance. 19 May 2021.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
