

Ischemic injury of the upper gastrointestinal tract after out-of-hospital cardiac arrest: a prospective, multicenter study
- PMID: 35287719
- PMCID: PMC8919548
- DOI: 10.1186/s13054-022-03939-9
Ischemic injury of the upper gastrointestinal tract after out-of-hospital cardiac arrest: a prospective, multicenter study
Abstract
Background: The consequences of cardiac arrest (CA) on the gastro-intestinal tract are poorly understood. We measured the incidence of ischemic injury in the upper gastro-intestinal tract after Out-of-hospital CA (OHCA) and determined the risk factors for and consequences of gastrointestinal ischemic injury according to its severity.
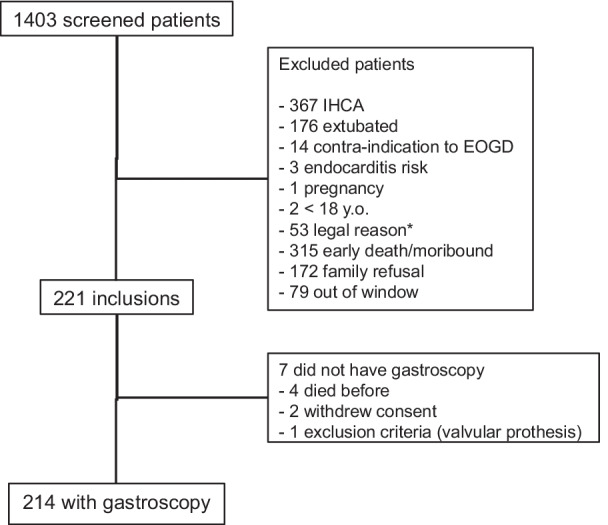
Methods: Prospective, non-controlled, multicenter study in nine ICUs in France and Belgium conducted from November 1, 2014 to November 30, 2018. Included patients underwent an esophago-gastro-duodenoscopy 2 to 4 d after OHCA if still intubated and the presence of ischemic lesions of the upper gastro-intestinal tract was determined by a gastroenterologist. Lesions were a priori defined as severe if there was ulceration or necrosis and moderate if there was mucosal edema or erythema. We compared clinical and cardiac arrest characteristics of three groups of patients (no, moderate, and severe lesions) and identified variables associated with gastrointestinal ischemic injury using multivariate regression analysis. We also compared the outcomes (organ failure during ICU stay and neurological status at hospital discharge) of the three groups of patients.
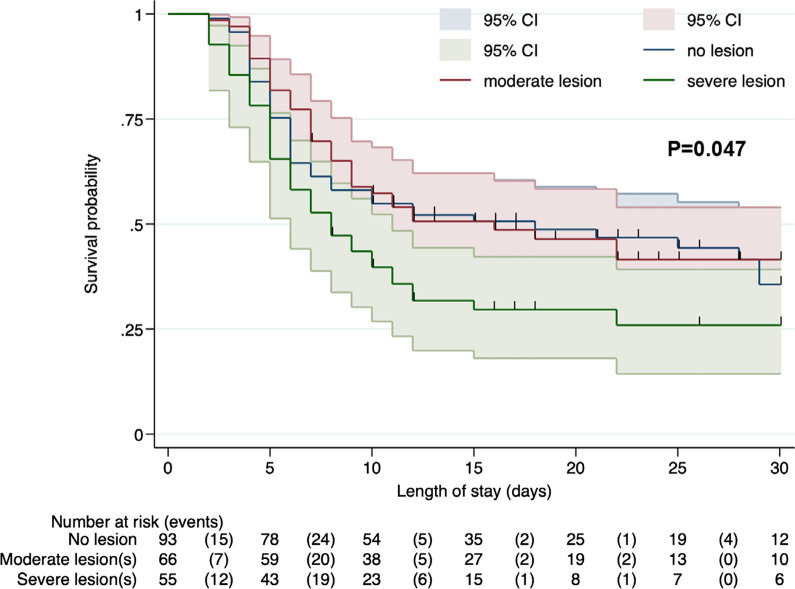
Results: Among the 214 patients included in the analysis, 121 (57%, 95% CI 50-63%) had an upper gastrointestinal ischemic lesion, most frequently on the fundus. Ischemic lesions were severe in 55/121 (45%) patients. In multivariate regression, higher adrenaline dose during cardiopulmonary resuscitation (OR 1.25 per mg (1.08-1.46)) was independently associated with increased odds of severe upper gastrointestinal ischemic lesions; previous proton pump inhibitor use (OR 0.40 (0.14-1.00)) and serum bicarbonate on day 1 (OR 0.89 (0.81-0.97)) were associated with lower odds of ischemic lesions. Patients with severe lesions had a higher SOFA score during the ICU stay and worse neurological outcome at hospital discharge.
Conclusions: More than half of the patients successfully resuscitated from OHCA had upper gastrointestinal tract ischemic injury. Presence of ischemic lesions was independently associated with the amount of adrenaline used during resuscitation. Patients with severe lesions had higher organ failure scores during the ICU stay and a worse prognosis. Clinical Trial Registration NCT02349074 .
Keywords: Cardiac arrest; Gastrointestinal tract; Gastroscopy; Gut; Ischemia/reperfusion; Mesenteric ischemia; Organ failure.
© 2022. The Author(s).
Conflict of interest statement
JM received congress reimbursement fees from CSL Behring & Biotest. DG received consultation fees from Transgene SA Illkirch Graffenstaden (France). AC received fees from Bard for lectures. Other authors have no disclosures.
Figures
References
-
- Adrie C, Adib-Conquy M, Laurent I, Monchi M, Vinsonneau C, Fitting C, et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation. 2002;106(5):562–568. doi: 10.1161/01.CIR.0000023891.80661.AD. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
