

COVID-19 and resilience of healthcare systems in ten countries
- PMID: 35288697
- PMCID: PMC9205770
- DOI: 10.1038/s41591-022-01750-1
COVID-19 and resilience of healthcare systems in ten countries
Abstract
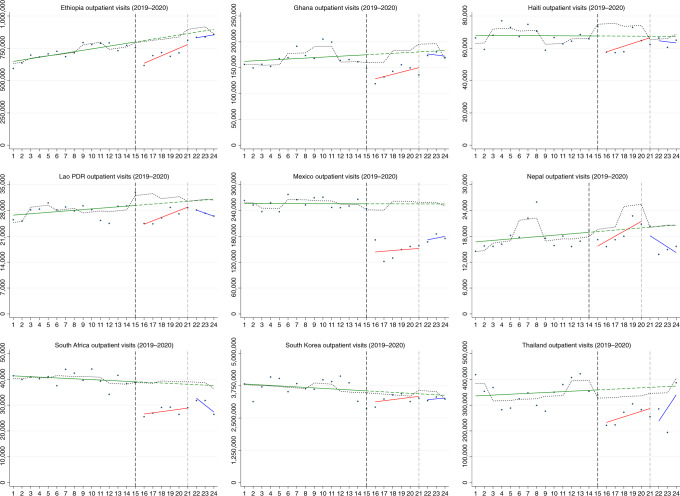
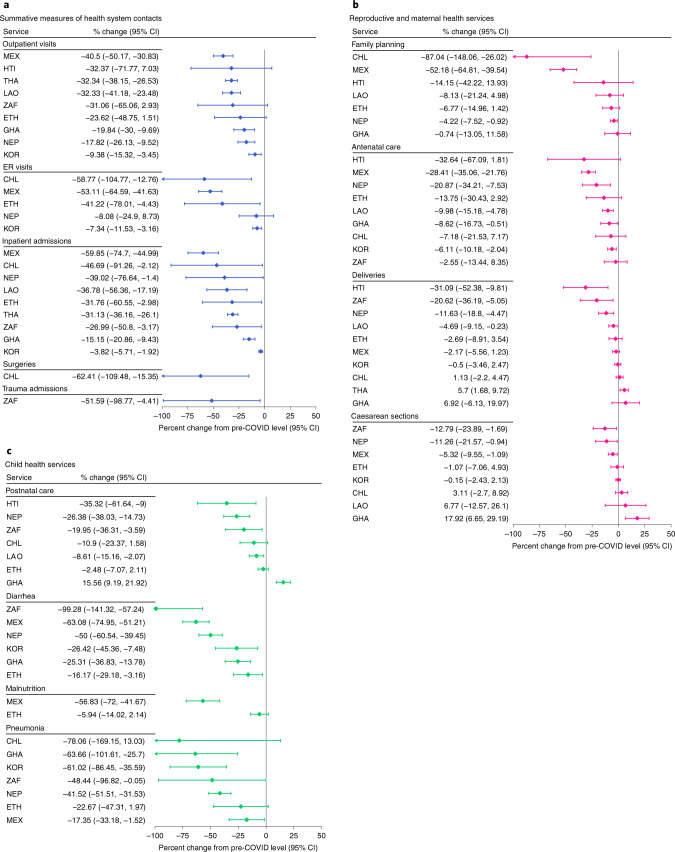
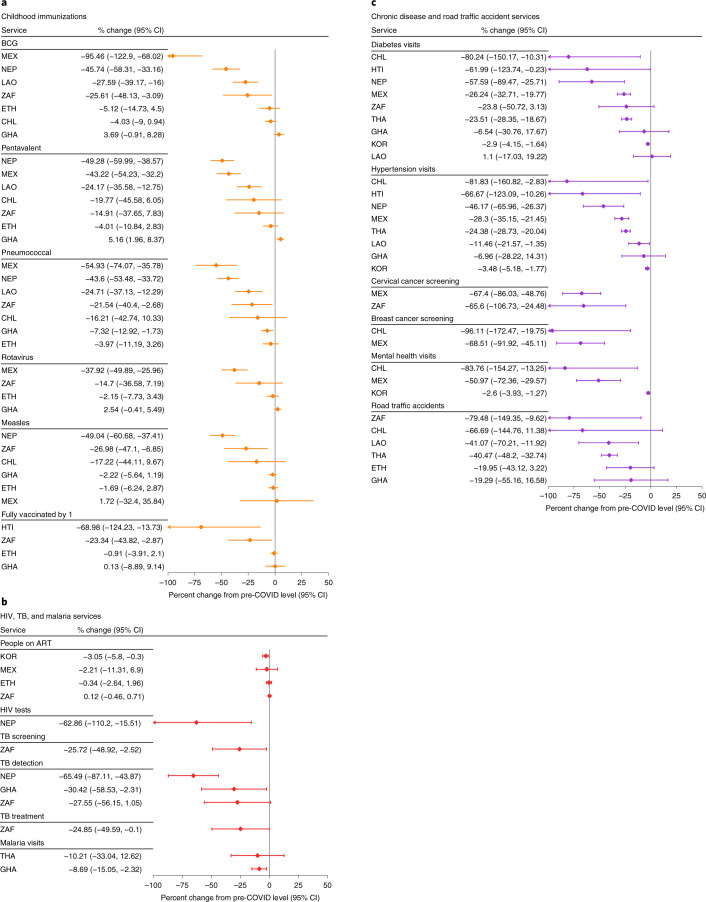
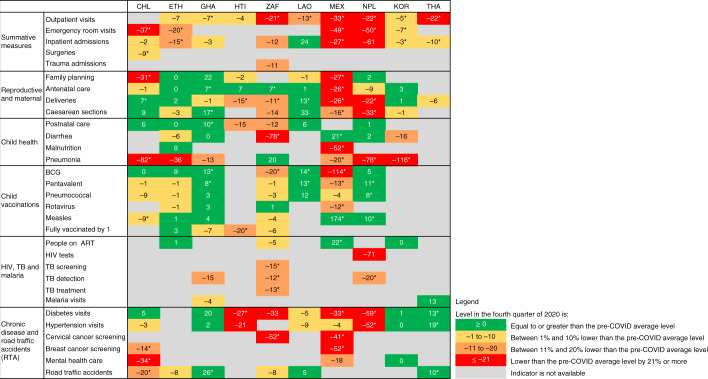
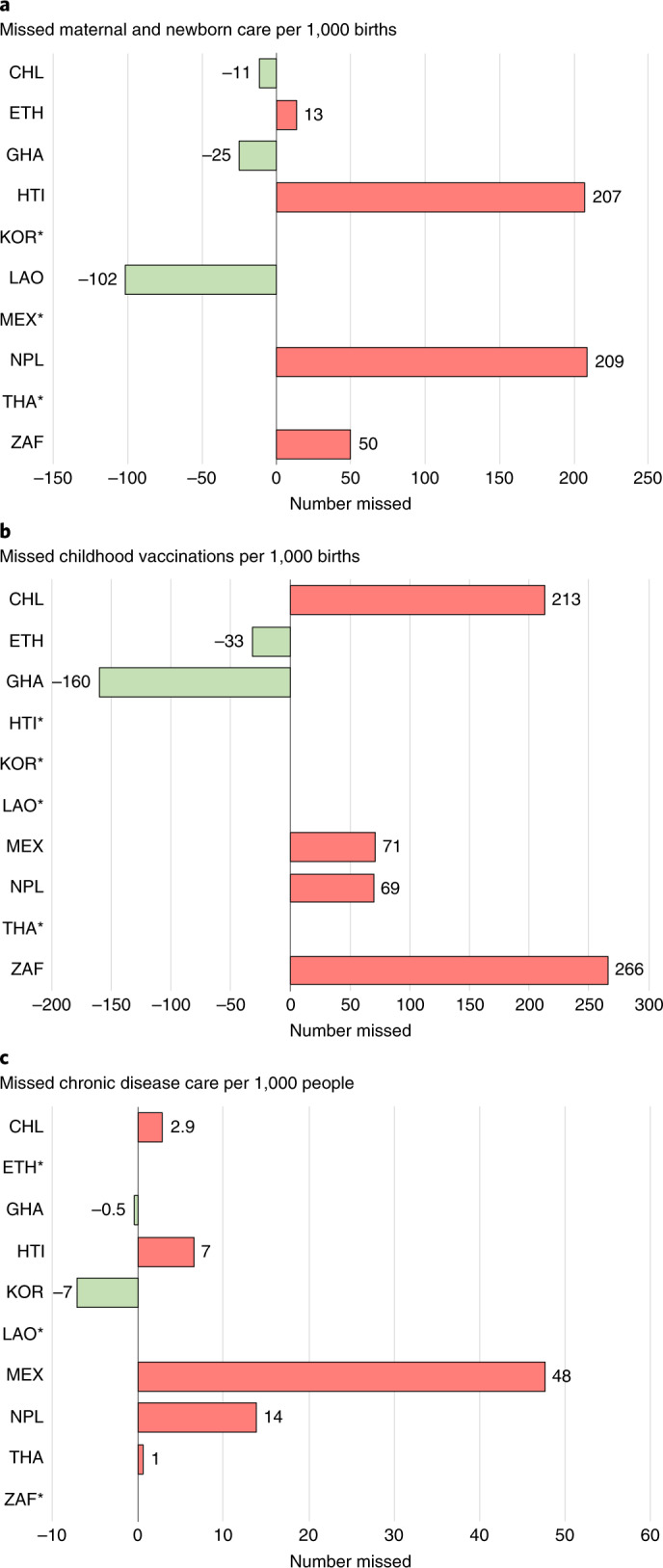
Declines in health service use during the Coronavirus Disease 2019 (COVID-19) pandemic could have important effects on population health. In this study, we used an interrupted time series design to assess the immediate effect of the pandemic on 31 health services in two low-income (Ethiopia and Haiti), six middle-income (Ghana, Lao People's Democratic Republic, Mexico, Nepal, South Africa and Thailand) and high-income (Chile and South Korea) countries. Despite efforts to maintain health services, disruptions of varying magnitude and duration were found in every country, with no clear patterns by country income group or pandemic intensity. Disruptions in health services often preceded COVID-19 waves. Cancer screenings, TB screening and detection and HIV testing were most affected (26-96% declines). Total outpatient visits declined by 9-40% at national levels and remained lower than predicted by the end of 2020. Maternal health services were disrupted in approximately half of the countries, with declines ranging from 5% to 33%. Child vaccinations were disrupted for shorter periods, but we estimate that catch-up campaigns might not have reached all children missed. By contrast, provision of antiretrovirals for HIV was not affected. By the end of 2020, substantial disruptions remained in half of the countries. Preliminary data for 2021 indicate that disruptions likely persisted. Although a portion of the declines observed might result from decreased needs during lockdowns (from fewer infectious illnesses or injuries), a larger share likely reflects a shortfall of health system resilience. Countries must plan to compensate for missed healthcare during the current pandemic and invest in strategies for better health system resilience for future emergencies.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






Comment in
-
The effect of the COVID-19 pandemic on the provision of outpatient clinic services in East Jerusalem hospitals: patients' perspectives.Front Public Health. 2023 Nov 24;11:1252449. doi: 10.3389/fpubh.2023.1252449. eCollection 2023. Front Public Health. 2023. PMID: 38074699 Free PMC article.
References
-
- Our World in Data. Statistics and Research: Coronavirus Pandemic (COVID-19), Country Profiles. https://ourworldindata.org/coronavirus#coronavirus-country-profiles2021 (2021).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
