

Pharmacological profile of asundexian, a novel, orally bioavailable inhibitor of factor XIa
- PMID: 35289054
- PMCID: PMC9313898
- DOI: 10.1111/jth.15700
Pharmacological profile of asundexian, a novel, orally bioavailable inhibitor of factor XIa
Erratum in
-
Corrigendum.J Thromb Haemost. 2022 Oct;20(10):2448. doi: 10.1111/jth.15845. J Thromb Haemost. 2022. PMID: 36123577 Free PMC article. No abstract available.
Abstract
Background: Activated coagulation factor XI (FXIa) contributes to the development and propagation of thrombosis but plays only a minor role in hemostasis; therefore, it is an attractive antithrombotic target.
Objectives: To evaluate the pharmacology of asundexian (BAY 2433334), a small molecule inhibitor targeting FXIa, in vitro and in various rabbit models.
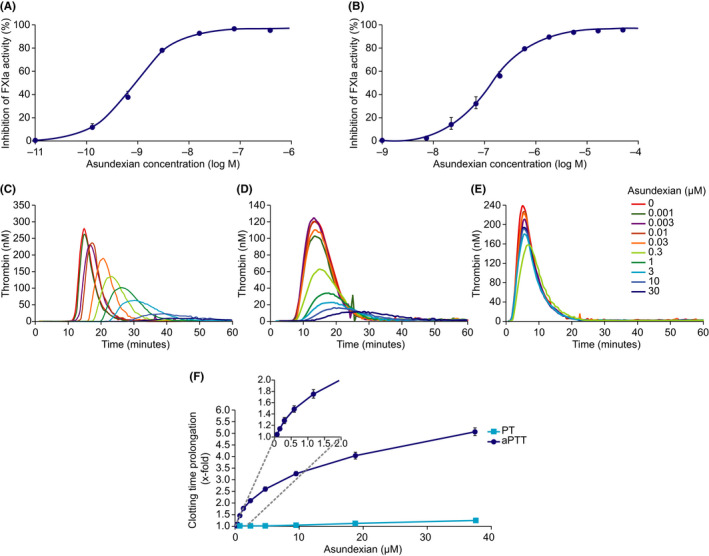
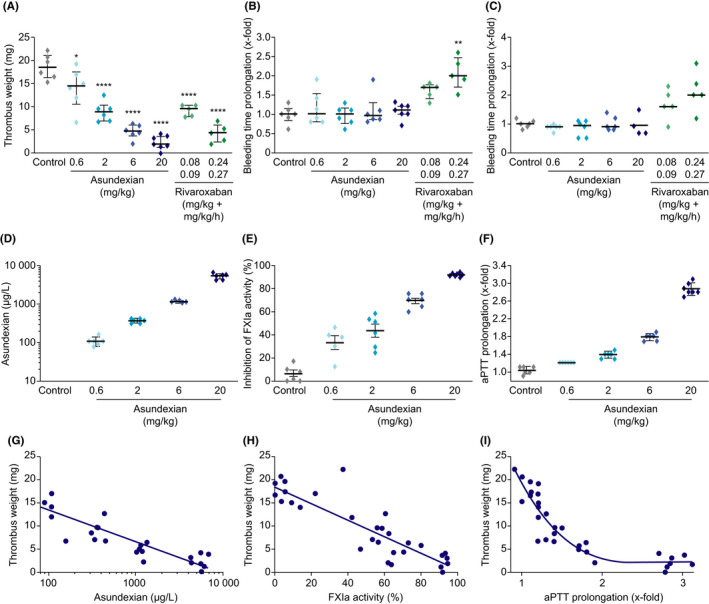
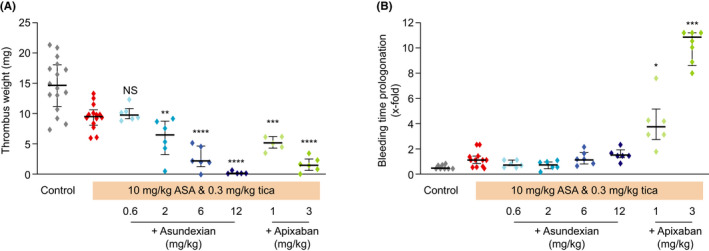
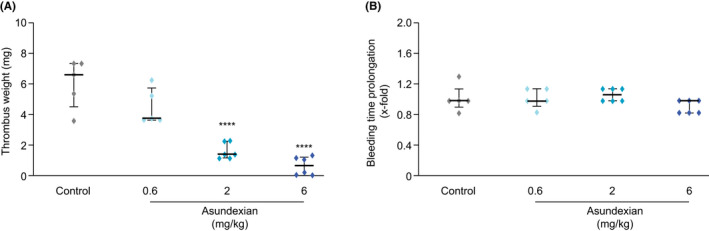
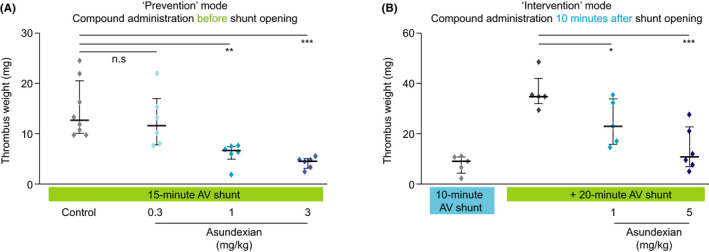
Methods: The effects of asundexian on FXIa activity, selectivity versus other proteases, plasma thrombin generation, and clotting assays were evaluated. Antithrombotic effects were determined in FeCl2 - and arterio-venous (AV) shunt models. Asundexian was administered intravenously or orally, before or during thrombus formation, and with or without antiplatelet drugs (aspirin and ticagrelor). Potential effects of asundexian on bleeding were evaluated in ear-, gum-, and liver injury models.
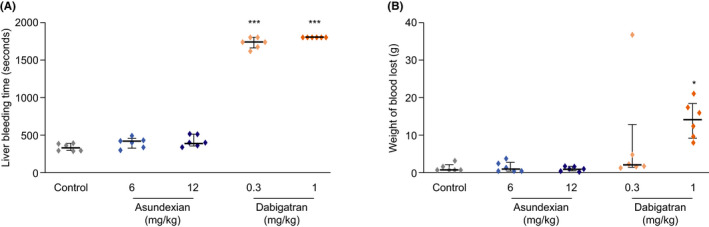
Results: Asundexian inhibited human FXIa with high potency and selectivity. It reduced FXIa activity, thrombin generation triggered by contact activation or low concentrations of tissue factor, and prolonged activated partial thromboplastin time in human, rabbit, and various other species, but not in rodents. In the FeCl2 -injury models, asundexian reduced thrombus weight versus control, and in the arterial model when added to aspirin and ticagrelor. In the AV shunt model, asundexian reduced thrombus weight when administered before or during thrombus formation. Asundexian alone or in combination with antiplatelet drugs did not increase bleeding times or blood loss in any of the models studied.
Conclusions: Asundexian is a potent oral FXIa inhibitor with antithrombotic efficacy in arterial and venous thrombosis models in prevention and intervention settings, without increasing bleeding.
Keywords: BAY 2433334; anticoagulant; asundexian; factor XIa inhibitor; thrombosis.
© 2022 Bayer AG. Journal of Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis.
Conflict of interest statement
Stefan Heitmeier, Adrian Tersteegen, Julia Glunz, Jan Stampfuss, Christoph Gerdes, Susanne Roehrig, and Julia Dietze‐Torres are all employees of Bayer AG. At the time this work was conducted, Mayken Visser and Volker Laux were both employees of Bayer AG but have subsequently left. Christoph Gerdes, Julia Glunz, Jan Stampfuss, Susanne Roehrig, and Adrian Tersteegen also own shares in Bayer AG.
Figures
Comment in
-
Commentary on "Pharmacological profile of asundexian, a novel, orally bioavailable inhibitor of factor XIa": Small molecule factor XIa inhibitor asundexian allows for safer anticoagulation.J Thromb Haemost. 2022 Jun;20(6):1309-1311. doi: 10.1111/jth.15722. J Thromb Haemost. 2022. PMID: 35596514 No abstract available.
References
-
- Weitz JI, Fredenburgh JC. 2017 scientific sessions sol sherry distinguished lecture in thrombosis. Arterioscler Thromb Vasc Biol. 2018;38(2):304‐310. - PubMed
-
- Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med. 2017;377(14):1319‐1330. - PubMed
-
- Bonaca MP, Bauersachs RM, Anand SS, et al. Rivaroxaban in peripheral artery disease after revascularization. N Engl J Med. 2020;382(21):1994‐2004. - PubMed
-
- Mega JL, Braunwald E, Wiviott SD, et al. Rivaroxaban in patients with a recent acute coronary syndrome. N Engl J Med. 2012;366(1):9‐19. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
