

Expiratory obstruction in patients with Duchenne muscular dystrophy under non-invasive ventilation: A step-by-step analysis of a new obstructive pattern
- PMID: 35289675
- PMCID: PMC8981231
- DOI: 10.1177/14799731211036901
Expiratory obstruction in patients with Duchenne muscular dystrophy under non-invasive ventilation: A step-by-step analysis of a new obstructive pattern
Abstract
Purpose: Non-invasive ventilation (NIV) is the reference standard for managing chronic hypoventilation in patients with Duchenne muscular dystrophy (DMD). In these patients, upper airway obstruction under NIV may compromise efficacy and adherence. We aim to describe a novel pattern of expiratory obstructive events occurring during nocturnal barometric NIV.
Methods: We retrospectively included all patients with DMD who underwent full-night polygraphy during NIV as part of their usual follow-up between May 2018 and July 2019.
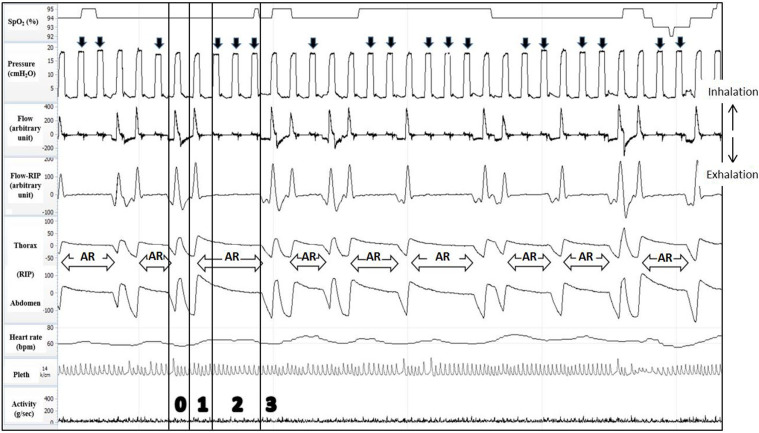
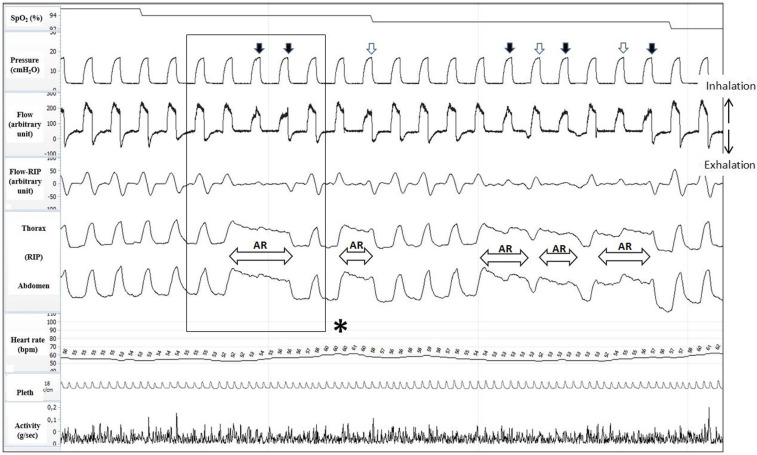
Results: We provide a step-by-step description of this previously undescribed pattern of obstruction. Expiratory obstructions lead to end-inspiratory breath-holding and impossibility to take another inspiratory breath with a barometric mode until expiration occurs. These events were observed in 4 (36%) of 11 DMD patients under barometric NIV.
Conclusion: Expiratory obstructions may be common in DMD patients receiving NIV and should be sought out routinely. This previously undescribed variant of obstructive event must be identified.
Keywords: Duchenne muscular dystrophy; neuromuscular diseases; non-invasive ventilation; patient–ventilator asynchrony; sleep apnea.
Conflict of interest statement
Figures

Similar articles
-
Determinants of usage and nonadherence to noninvasive ventilation in children and adults with Duchenne muscular dystrophy.J Clin Sleep Med. 2021 Oct 1;17(10):1973-1980. doi: 10.5664/jcsm.9400. J Clin Sleep Med. 2021. PMID: 33949945 Free PMC article.
-
Understanding adherence to noninvasive ventilation in youth with Duchenne muscular dystrophy.Pediatr Pulmonol. 2019 Dec;54(12):2035-2043. doi: 10.1002/ppul.24484. Epub 2019 Sep 1. Pediatr Pulmonol. 2019. PMID: 31475475 Free PMC article.
-
Impact of Noninvasive Ventilation on Lung Volumes and Maximum Respiratory Pressures in Duchenne Muscular Dystrophy.Respir Care. 2016 Nov;61(11):1530-1535. doi: 10.4187/respcare.04703. Epub 2016 Oct 18. Respir Care. 2016. PMID: 27794082
-
Lifetime Care of Duchenne Muscular Dystrophy.Sleep Med Clin. 2020 Dec;15(4):485-495. doi: 10.1016/j.jsmc.2020.08.011. Epub 2020 Oct 5. Sleep Med Clin. 2020. PMID: 33131659 Free PMC article. Review.
-
The growing role of noninvasive ventilation in patients requiring prolonged mechanical ventilation.Respir Care. 2012 Jun;57(6):900-18; discussion 918-20. doi: 10.4187/respcare.01692. Respir Care. 2012. PMID: 22663966 Review.
References
-
- Aboussouan LS, Mireles-Cabodevila E. Sleep-disordered breathing in neuromuscular disease. Chest 2017; 152(4): 880–892. - PubMed
-
- Gonzalez-Bermejo J, Perrin C, Janssens JP, et al. Proposal for a systematic analysis of polygraphy or polysomnography for identifying and scoring abnormal events occurring during non-invasive ventilation. Thorax 2012; 67(6): 546–552. - PubMed
-
- Aarrestad S, Qvarfort M, Kleiven AL, et al. Sleep related respiratory events during non-invasive ventilation of patients with chronic hypoventilation. Respir Med 2017; 132: 210–216. - PubMed
-
- Schellhas V, Glatz C, Beecken I, et al. Upper airway obstruction induced by non-invasive ventilation using an oronasal interface. Sleep Breath 2018; 22(3): 781–788. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
