

Ex vivo comparison of 3 Tesla magnetic resonance imaging and multidetector computed tomography arthrography to identify artificial soft tissue lesions in equine stifles
- PMID: 35289943
- PMCID: PMC9314790
- DOI: 10.1111/vsu.13798
Ex vivo comparison of 3 Tesla magnetic resonance imaging and multidetector computed tomography arthrography to identify artificial soft tissue lesions in equine stifles
Abstract
Objective: To determine the diagnostic performance of computed tomographic arthrography (CTA) and 3 Tesla magnetic resonance imaging (MRI) for detecting artificial meniscal, meniscotibial ligament (MTL) lesions and cruciate ligament (CL) lesions in horses.
Study design: Ex vivo controlled laboratory study.
Animals: Nineteen stifles from adult horses.
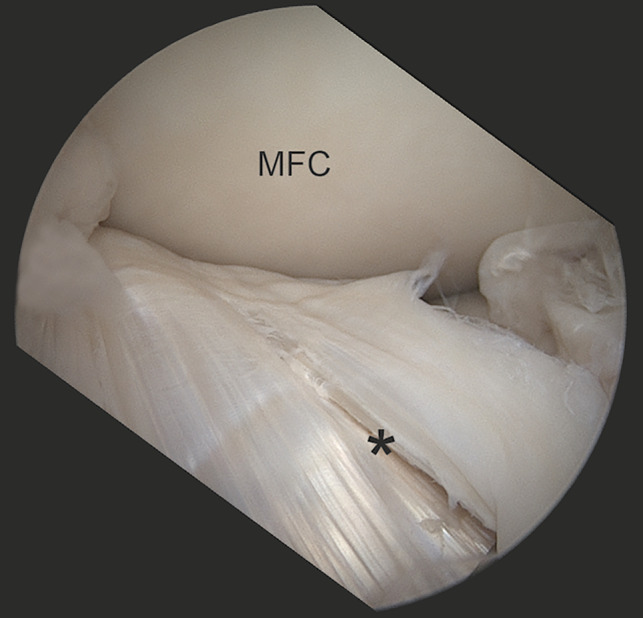
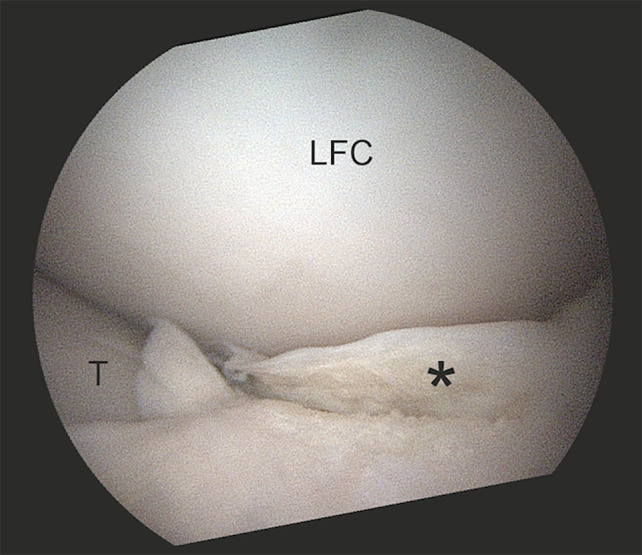
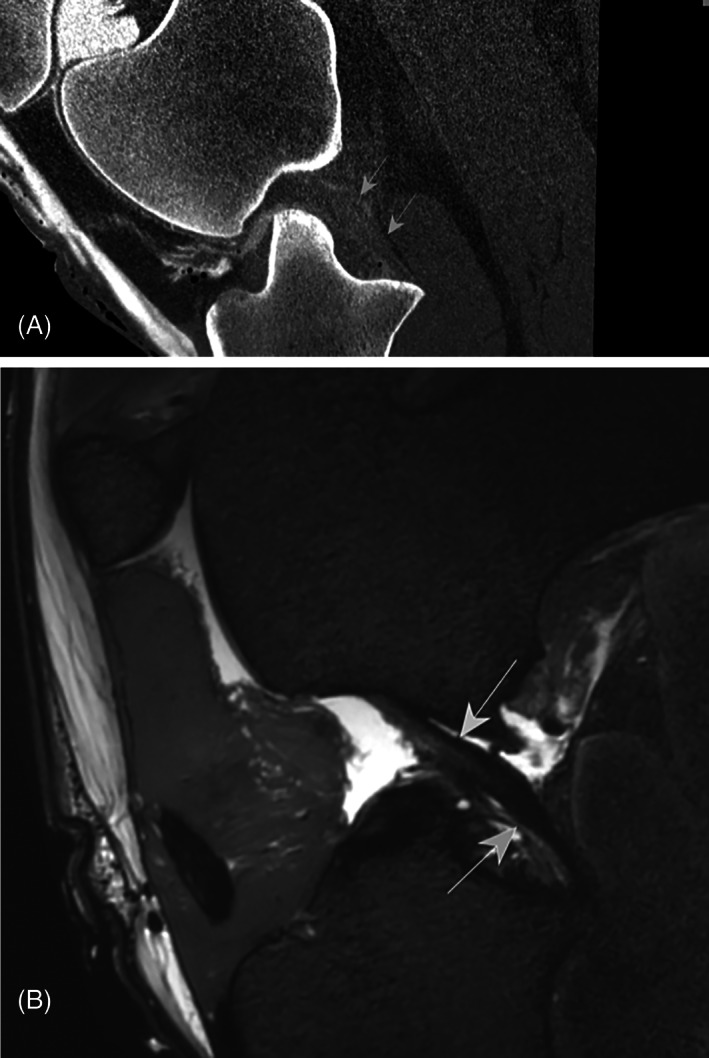
Methods: Stablike defects (n = 84) (16 mm long, 10 mm deep) were created in the menisci (n = 35), CLs (n = 24), and MTLs (n = 25) via arthroscopy prior to MRI and CTA (80 mL contrast at 85 mg/mL per joint). Two radiologists, unaware of the lesions, reached a consensus regarding the presence of lesions, based on 2 reviews of each study. Sensitivity and specificity of MRI and CTA were determined using arthroscopy as a reference and compared with McNemar's tests.
Results: The sensitivity and specificity of MRI (41% and 86% respectively) and CTA (32% and 90% respectively) did not differ (P = .65). The sensitivity (MRI: 24%-50%; CTA:19%-40%) and specificity (MRI: 75%-92%; CTA 75%-100%) of imaging modalities did not differ when detecting lesions of the menisci, MTLs, and CLs (P = .1-1.0). The highest sensitivities were achieved when MTLs were evaluated with MRI (50%) and CLs with both modalities (40%).
Conclusions: The diagnostic performance of CTA was comparable with that of MRI, with a low to moderate sensitivity and high specificity.
Clinical significance: Computed tomographic arthrography should be considered as an adjunct to diagnose CL injuries. This is important for equine clinicians, as the CL cannot be visualized adequately using basic imaging techniques preoperatively.
© 2022 The Authors. Veterinary Surgery published by Wiley Periodicals LLC on behalf of American College of Veterinary Surgeons.
Conflict of interest statement
The authors declare no conflict of interest related to this report.
Figures


References
-
- Singer ER, Barnes J, Saxby F, Murray JK. Injuries in the event horse: training versus competition. Vet J. 2008;175:76‐81. - PubMed
-
- Jeffcott L, Kold S. Stifle lameness in the horse: a survey of 86 referred cases. Equine Vet J. 1982;14:31‐39. - PubMed
-
- Dyson SJ. Lameness associated with the stifle and pelvic regions. Proc AAEP. 2002;48.387‐411.
-
- Cohen JM, Richardson DW, McKnight AL, et al. Long‐term outcome in 44 horses with stifle lameness after arthroscopic exploration and debridement. Vet Surg. 2009;38:543‐551. - PubMed
-
- Walmsley JP, Phillips TJ. Townsend: meniscal tears in horses: an evaluation of clinical signs and arthroscopic treatment of 80 cases. Equine Vet J. 2003;35:402‐406. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
