

SSEP N20 and P25 amplitudes predict poor and good neurologic outcomes after cardiac arrest
- PMID: 35290522
- PMCID: PMC8924339
- DOI: 10.1186/s13613-022-00999-6
SSEP N20 and P25 amplitudes predict poor and good neurologic outcomes after cardiac arrest
Abstract
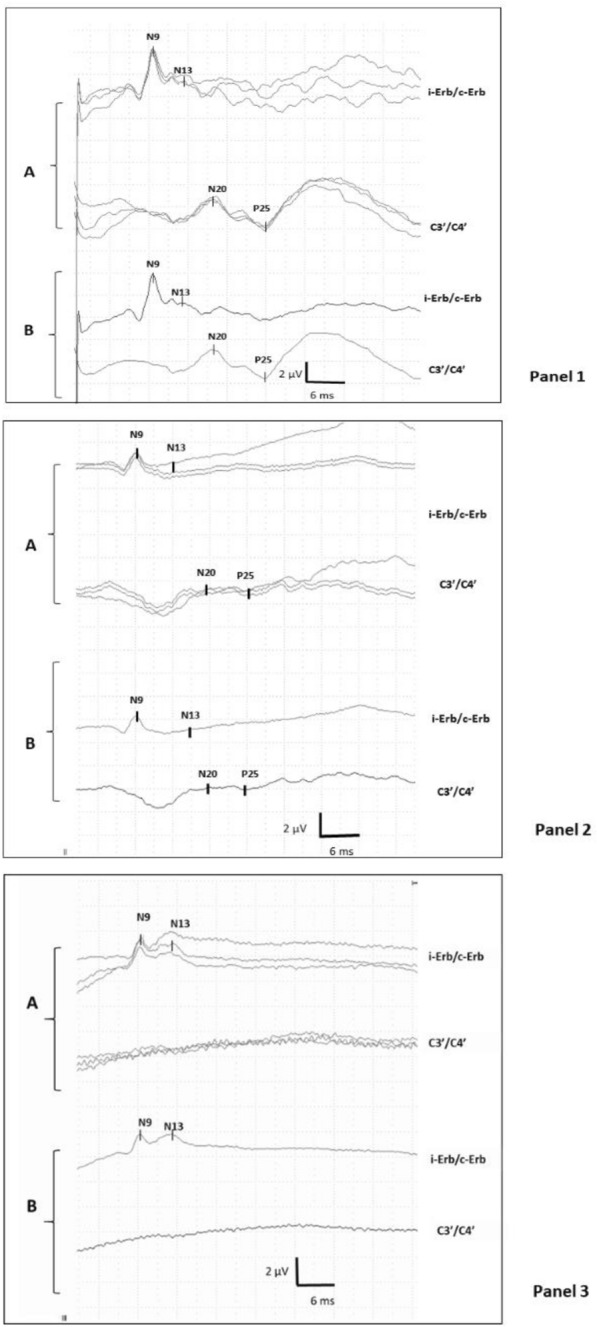
Background: To assess in comatose patients after cardiac arrest (CA) if amplitudes of two somatosensory evoked potentials (SSEP) responses, namely, N20-baseline (N20-b) and N20-P25, are predictive of neurological outcome.
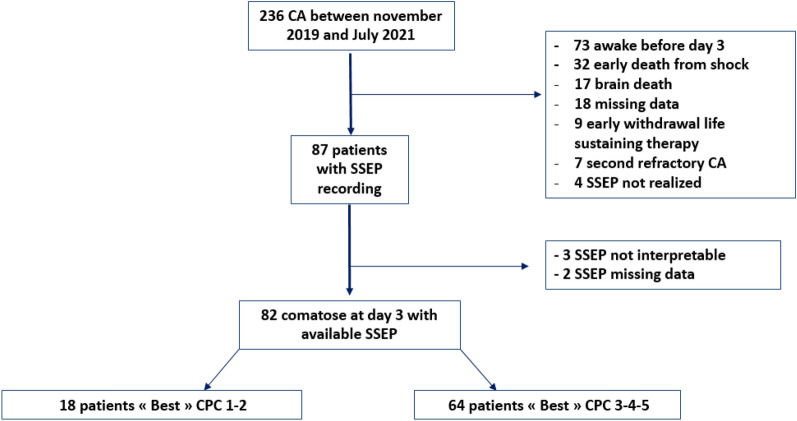
Methods: Monocentric prospective study in a tertiary cardiac center between Nov 2019 and July-2021. All patients comatose at 72 h after CA with at least one SSEP recorded were included. The N20-b and N20-P25 amplitudes were automatically measured in microvolts (µV), along with other recommended prognostic markers (status myoclonus, neuron-specific enolase levels at 2 and 3 days, and EEG pattern). We assessed the predictive value of SSEP for neurologic outcome using the best Cerebral Performance Categories (CPC1 or 2 as good outcome) at 3 months (main endpoint) and 6 months (secondary endpoint). Specificity and sensitivity of different thresholds of SSEP amplitudes, alone or in combination with other prognostic markers, were calculated.
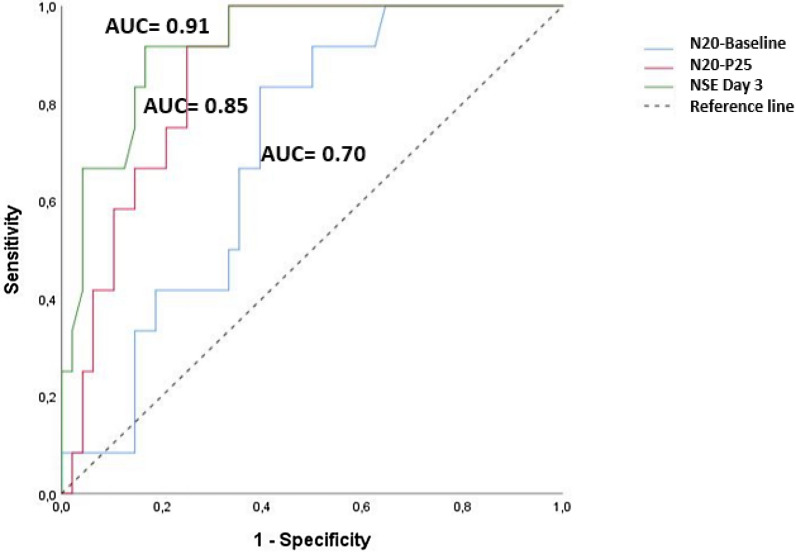
Results: Among 82 patients, a poor outcome (CPC 3-5) was observed in 78% of patients at 3 months. The median time to SSEP recording was 3(2-4) days after CA, with a pattern "bilaterally absent" in 19 patients, "unilaterally present" in 4, and "bilaterally present" in 59 patients. The median N20-b amplitudes were different between patients with poor and good outcomes, i.e., 0.93 [0-2.05]µV vs. 1.56 [1.24-2.75]µV, respectively (p < 0.0001), as the median N20-P25 amplitudes (0.57 [0-1.43]µV in poor outcome vs. 2.64 [1.39-3.80]µV in good outcome patients p < 0.0001). An N20-b > 2 µV predicted good outcome with a specificity of 73% and a moderate sensitivity of 39%, although an N20-P25 > 3.2 µV was 93% specific and only 30% sensitive. A low voltage N20-b < 0.88 µV and N20-P25 < 1 µV predicted poor outcome with a high specificity (sp = 94% and 93%, respectively) and a moderate sensitivity (se = 50% and 66%). Association of "bilaterally absent or low voltage SSEP" patterns increased the sensitivity significantly as compared to "bilaterally absent" SSEP alone (se = 58 vs. 30%, p = 0.002) for prediction of poor outcome.
Conclusion: In comatose patient after CA, both N20-b and N20-P25 amplitudes could predict both good and poor outcomes with high specificity but low to moderate sensitivity. Our results suggest that caution is needed regarding SSEP amplitudes in clinical routine, and that these indicators should be used in a multimodal approach for prognostication after cardiac arrest.
Keywords: Cardiac arrest; EEG; NSE; Neuroprognostication; Persistent coma; Prognosis; Somato sensory evoked potential; Status myoclonus.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Soar J, Maconochie I, Wyckoff MH, Olasveengen TM, Singletary EM, Greif R, et al. International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations: summary from the basic life support; advanced life support; pediatric life support; neonatal life support; education, implementation, and teams; and first aid task forces. Circulation. 2019;2019:140. doi: 10.1161/CIR.0000000000000734. - DOI - PubMed
-
- Comanducci A, Boly M, Claassen J, De Lucia M, Gibson RM, Juan E, et al. Clinical and advanced neurophysiology in the prognostic and diagnostic evaluation of disorders of consciousness: review of an IFCN-endorsed expert group. Clin Neurophysiol. 2020;131:2736–2765. doi: 10.1016/j.clinph.2020.07.015. - DOI - PubMed
LinkOut - more resources
Full Text Sources
