

Efficacy of probiotics or synbiotics for critically ill adult patients: a systematic review and meta-analysis of randomized controlled trials
- PMID: 35291228
- PMCID: PMC8918756
- DOI: 10.1093/burnst/tkac004
Efficacy of probiotics or synbiotics for critically ill adult patients: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Microbial dysbiosis in critically ill patients is a leading cause of mortality and septic complications. Probiotics and synbiotics have emerged as novel therapy on gut microbiota to prevent septic complications. However, current evidence on their effects is conflicting. This work aims to systematically review the impact of probiotics or synbiotics in critically ill adult patients.
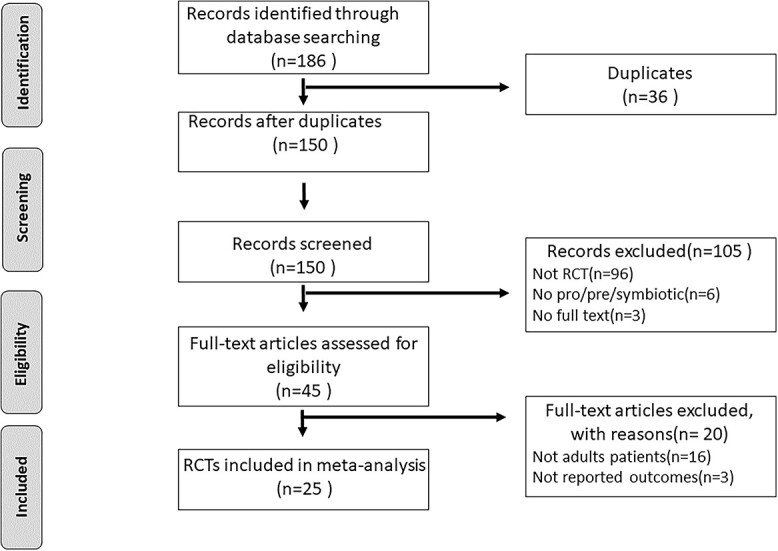
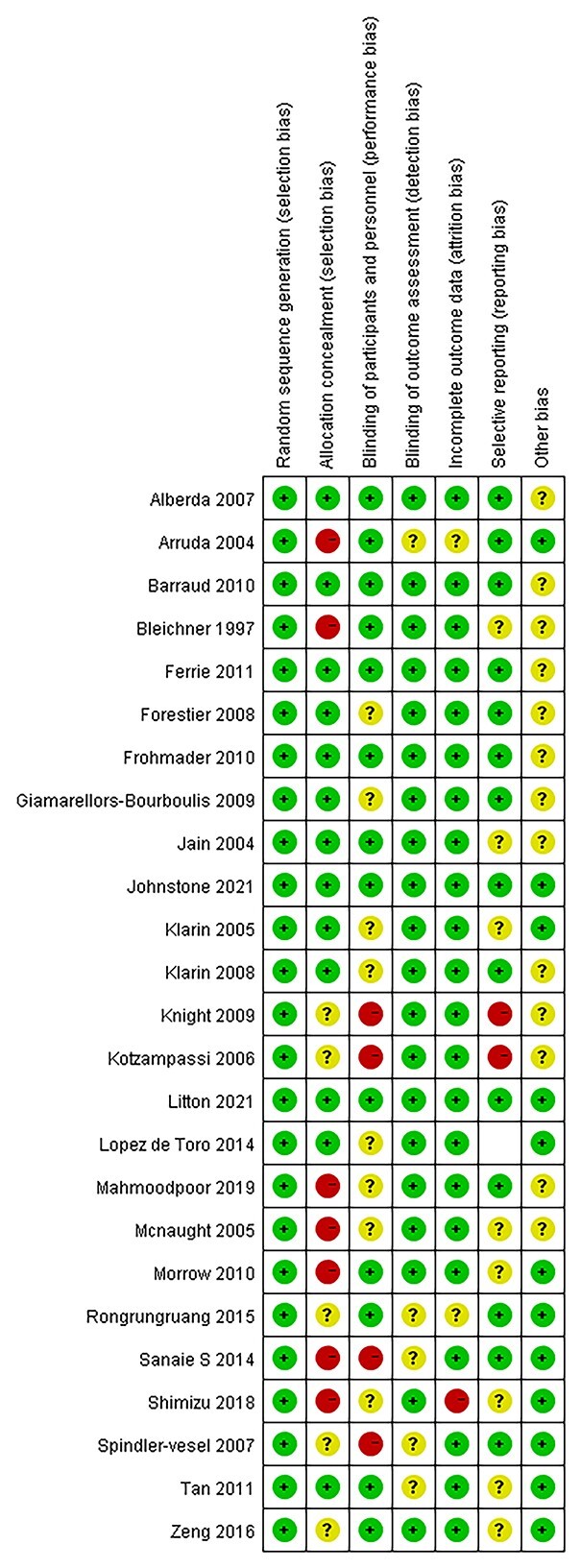
Methods: A comprehensive search of the PubMed, CBM, Embase, CENTRAL, ISI, and CNKI databases was performed to identify randomized controlled trials that evaluate probiotics or synbiotics in critically ill patients. The quality assessment was based on the modified Jadad's score scale and the Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1. The major outcome measure was mortality. Secondary outcomes included incidence of septic complications, sepsis incidence, length of intensive care unit (ICU) stay, incidence of non-septic complication, and ventilator day. Data synthesis was conduct by Review Manager 5.4.
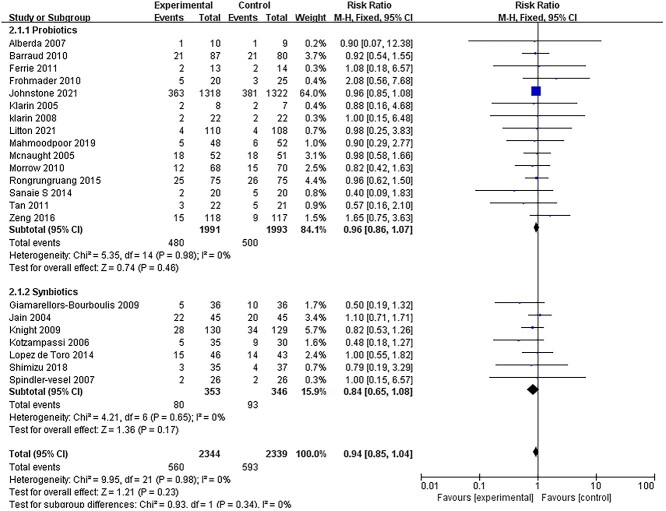
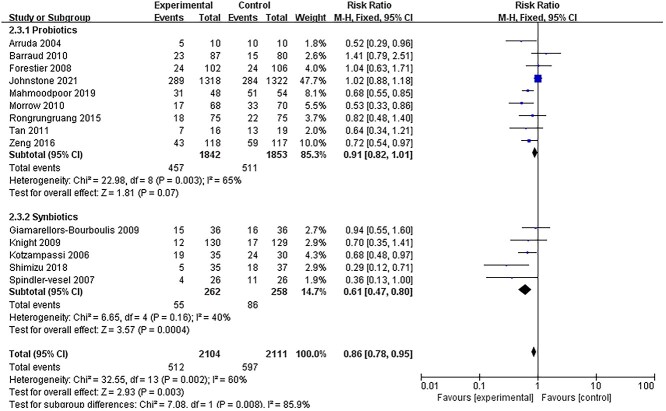
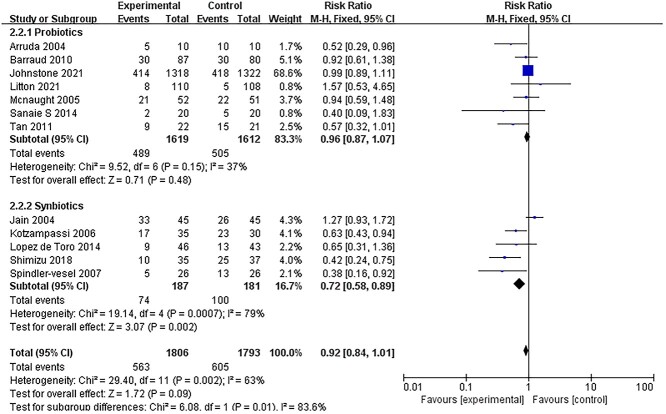
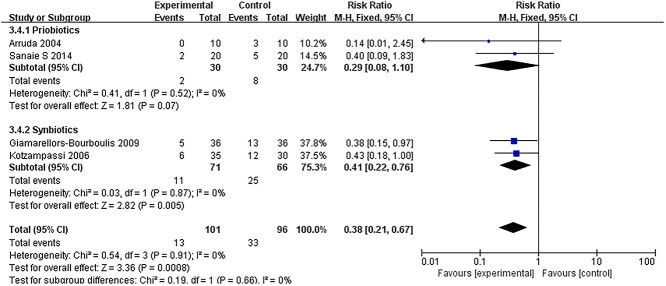
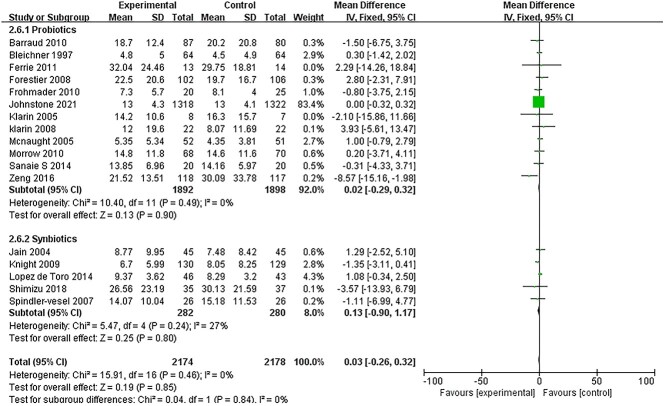
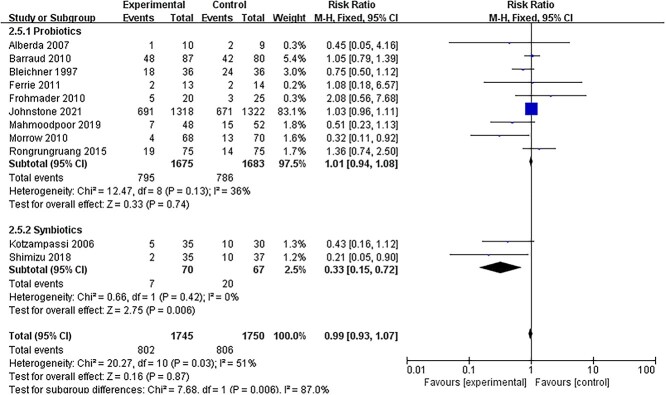
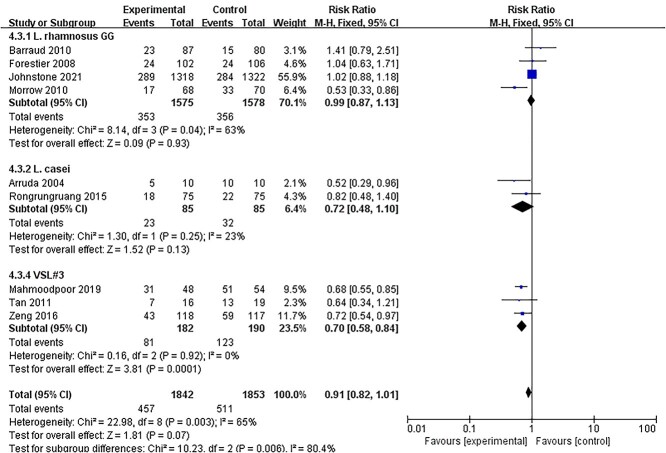
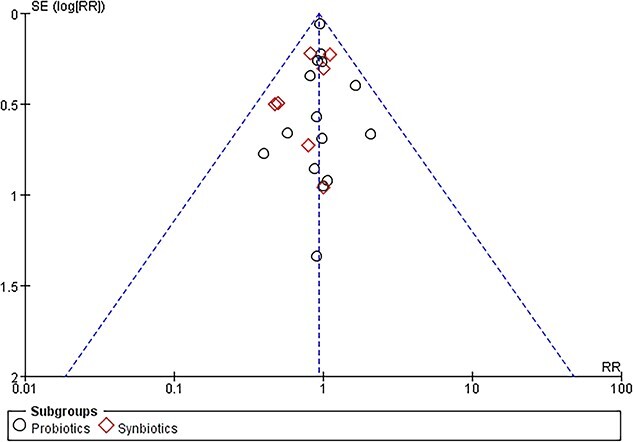
Results: A total of 25 randomized controlled trials reporting on 5049 critically ill patients were included. In the intervention group, 2520 participants received probiotics or synbiotics, whereas 2529 participants received standard care or placebo. Pooling data from randomized controlled trials demonstrated a significant reduction in the incidence of ventilator-associated pneumonia (VAP) in the treatment group [(risk ratio (RR) 0.86; 95% confidence interval (CI): 0.78-0.95; p < 0.003, I2 = 85%)]. However, in the subgroup analysis, the reduction of incidence of VAP was only significant in patients receiving synbiotics (RR = 0.61, 95% CI: 0.47-0.80, p = 0.0004, I2 = 40%) and not significant in those receiving only probiotics (RR = 0.91, 95% CI: 0.82-1.01, p = 0.07, I2 = 65%). Moreover, sepsis incidence of critically ill patients was only significantly reduced by the addition of synbiotics (RR = 0.41; 95% CI: 0.22-0.72, p = 0.005, I2 = 0%). The incidence of ICU-acquired infections was significantly reduced by the synbiotics therapy (RR = 0.72; 95% CI: 0.58-0.89, p = 0.0007, I2 = 79%). There was no significant difference in mortality, diarrhea, or length of ICU stay between the treatment and control groups.
Conclusions: Synbiotics is an effective and safe nutrition therapy in reducing septic complications in critically ill patients. However, in such patients, administration of probiotics alone compared with placebo resulted in no difference in the septic complications.
Keywords: Critically ill patients; Meta-analysis; Mortality; Probiotics; Synbiotics; Systematic review; Ventilator-associated pneumonia.
© The Author(s) 2022. Published by Oxford University Press.
Figures
Similar articles
-
Efficacy of probiotics or synbiotics in critically ill patients: A systematic review and meta-analysis.Clin Nutr ESPEN. 2024 Feb;59:48-62. doi: 10.1016/j.clnesp.2023.11.003. Epub 2023 Nov 8. Clin Nutr ESPEN. 2024. PMID: 38220407
-
Benefits and harm of probiotics and synbiotics in adult critically ill patients. A systematic review and meta-analysis of randomized controlled trials with trial sequential analysis.Clin Nutr. 2023 Apr;42(4):519-531. doi: 10.1016/j.clnu.2023.01.019. Epub 2023 Feb 7. Clin Nutr. 2023. PMID: 36857961
-
Synbiotic Therapy Prevents Nosocomial Infection in Critically Ill Adult Patients: A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials Based on a Bayesian Framework.Front Med (Lausanne). 2021 Jul 15;8:693188. doi: 10.3389/fmed.2021.693188. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34336896 Free PMC article.
-
Perioperative Probiotics or Synbiotics in Adults Undergoing Elective Abdominal Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials.Ann Surg. 2020 Jun;271(6):1036-1047. doi: 10.1097/SLA.0000000000003581. Ann Surg. 2020. PMID: 31469748
-
The effectiveness of probiotics or synbiotics in the prevention and treatment of diarrhea among critically ill adults: A systematic review and meta-analysis.Clin Nutr ESPEN. 2025 Feb;65:218-226. doi: 10.1016/j.clnesp.2024.11.025. Epub 2024 Dec 3. Clin Nutr ESPEN. 2025. PMID: 39638033
Cited by
-
[Immunomodulation by nutritional intervention in critically ill patients].Anaesthesiologie. 2023 Apr;72(4):229-244. doi: 10.1007/s00101-023-01258-4. Epub 2023 Feb 16. Anaesthesiologie. 2023. PMID: 36797533 Free PMC article. Review. German.
-
Postbiotics as potential new therapeutic agents for sepsis.Burns Trauma. 2023 Jun 15;11:tkad022. doi: 10.1093/burnst/tkad022. eCollection 2023. Burns Trauma. 2023. PMID: 37334140 Free PMC article. Review.
-
Why Give My Surgical Patients Probiotics.Nutrients. 2022 Oct 19;14(20):4389. doi: 10.3390/nu14204389. Nutrients. 2022. PMID: 36297073 Free PMC article.
-
The impact of gut microbiota changes on the intestinal mucus barrier in burned mice: a study using 16S rRNA and metagenomic sequencing.Burns Trauma. 2023 Dec 19;11:tkad056. doi: 10.1093/burnst/tkad056. eCollection 2023. Burns Trauma. 2023. PMID: 38130728 Free PMC article.
-
Optimization of Therapy and the Risk of Probiotic Use during Antibiotherapy in Septic Critically Ill Patients: A Narrative Review.Medicina (Kaunas). 2023 Feb 28;59(3):478. doi: 10.3390/medicina59030478. Medicina (Kaunas). 2023. PMID: 36984479 Free PMC article. Review.
References
-
- Bateman BT, Schmidt U, Berman MF, Bittner EA. Temporal trends in the epidemiology of severe postoperative sepsis after elective surgery: a large, nationwide sample. Anesthesiology. 2010;112:917–25. - PubMed
-
- Martin GS, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–54. - PubMed
-
- Kreymann KG, Berger MM, Deutz NE, Hiesmayr M, Jolliet P, Kazandjiev G, et al. . ESPEN guidelines on enteral nutrition: intensive care. Clin Nutr. 2006;25:210–23. - PubMed
-
- Biancone L, Monteleone I, Del Vecchio BG, Vavassori P, Pallone F. Resident bacterial flora and immune system. Dig Liver Dis. 2002;34:S37–43. - PubMed
LinkOut - more resources
Full Text Sources
