

Distal Radioulnar Joint Instability: Diagnosis and Treatment
- PMID: 35291239
- PMCID: PMC8889419
- DOI: 10.22038/ABJS.2021.57194.2833
Distal Radioulnar Joint Instability: Diagnosis and Treatment
Abstract
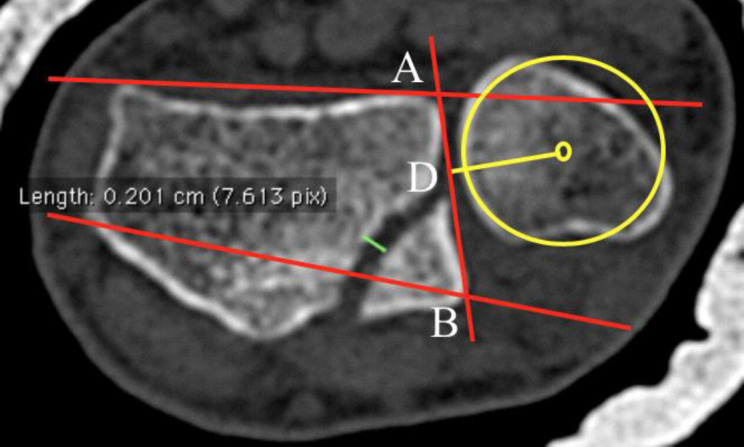
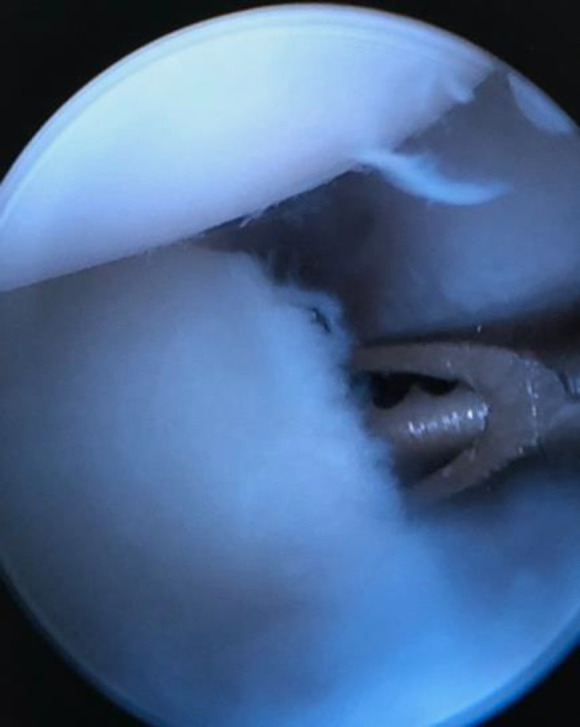
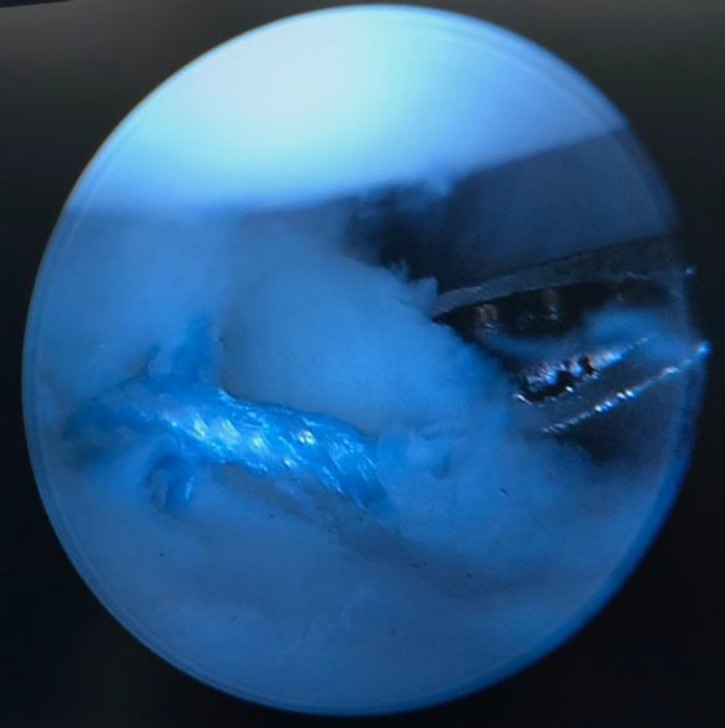
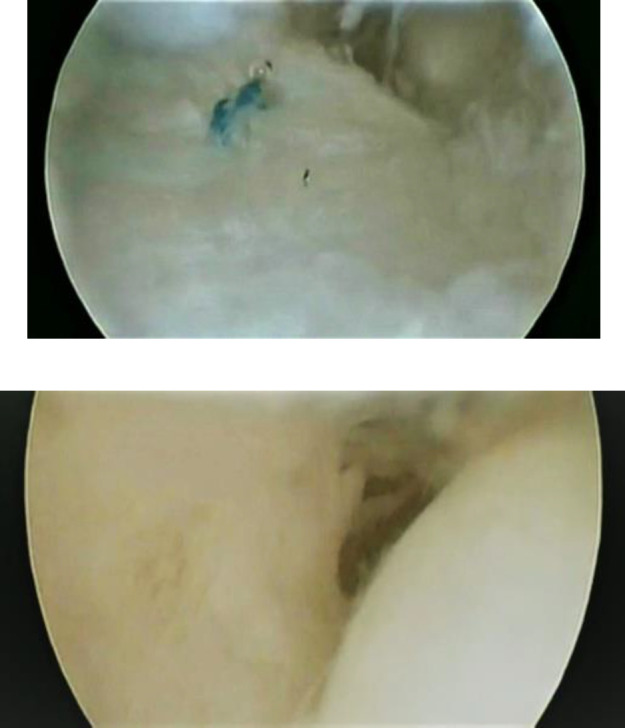
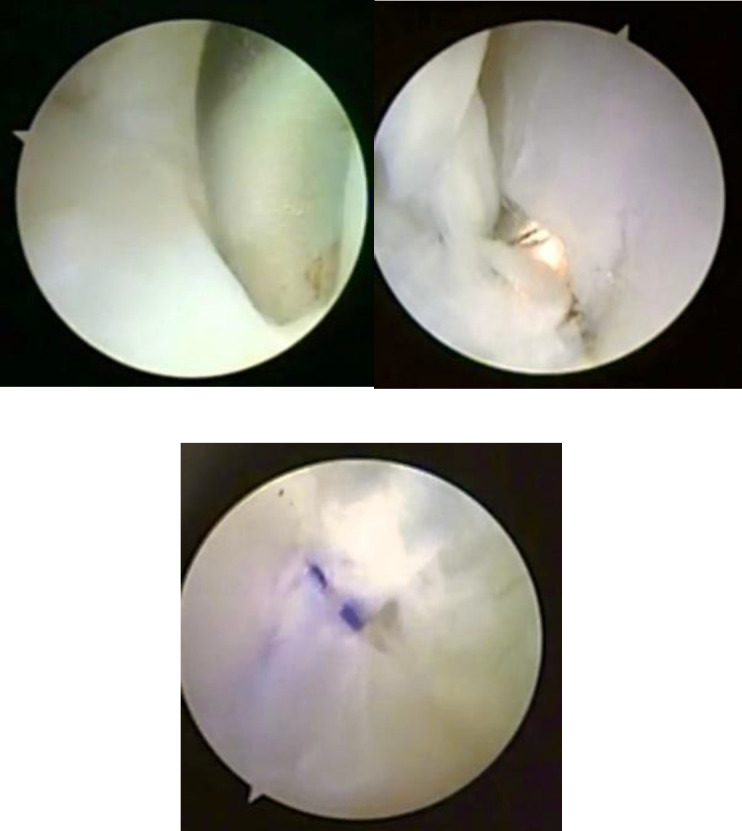
Distal radioulnar joint (DRUJ) instability and triangular fibrocartilage complex (TFCC) tears are more usual than estimated and are frequently overlooked. Diagnosis is often clinical, which can be confirmed using computed tomography (CT) scan and magnetic resonance imaging (MRI). In doubtful cases, bilateral computed tomography in neutral forearm rotation, supination, and pronation should also be performed. Wrist arthroscopy can be diagnostic and therapeutic for ulnar-sided wrist pain. Two systematic reviews showed equivalent outcomes between open and arthroscopic repair of the TFCC. There is scant proof to advise one technique over the other in clinical practice. TFCC repair and reconstruction are contraindicated when there is a bony deformation of the radius or ulna or osteoarthritis of the DRUJ. With the advancement of implant arthroplasty, salvage procedures are less desirable. Constrained distal radioulnar arthroplasty is stable, and the longevity is encouraging.
Keywords: Distal radioulnar joint; Instability; Treatment; Triangular fibrocartilage complex.
Figures








Similar articles
-
Effect of Volarly Angulated Distal Radius Fractures on Forearm Rotation and Distal Radioulnar Joint Kinematics.J Hand Surg Am. 2015 Nov;40(11):2236-42. doi: 10.1016/j.jhsa.2015.07.034. Epub 2015 Sep 26. J Hand Surg Am. 2015. PMID: 26409579
-
Biomechanical Analysis of Capsular Repair Versus Arthrex TFCC Ulnar Tunnel Repair for Triangular Fibrocartilage Complex Tears.Hand (N Y). 2019 Jul;14(4):547-553. doi: 10.1177/1558944717750920. Epub 2018 Jan 11. Hand (N Y). 2019. PMID: 29322875 Free PMC article.
-
Patients With Triangular Fibrocartilage Complex Injuries and Distal Radioulnar Joint Instability Gain Improved Forearm Peak Pronation and Supination Torque After Reinsertion.Hand (N Y). 2020 Mar;15(2):281-286. doi: 10.1177/1558944718793198. Epub 2018 Aug 6. Hand (N Y). 2020. PMID: 30081654 Free PMC article.
-
Distal radioulnar joint instability: current concepts of treatment.Arch Orthop Trauma Surg. 2020 May;140(5):639-650. doi: 10.1007/s00402-020-03371-0. Epub 2020 Mar 19. Arch Orthop Trauma Surg. 2020. PMID: 32193678 Review.
-
Acute Distal Radioulnar Joint Instability: Evaluation and Treatment.Hand Clin. 2020 Nov;36(4):429-441. doi: 10.1016/j.hcl.2020.07.005. Epub 2020 Sep 2. Hand Clin. 2020. PMID: 33040955 Review.
Cited by
-
The Unpredictable Palmaris Longus Tendon Variation in Distal Radio-Ulnar Joint Reconstruction: A Technical Consideration for Undersized Graft.Orthop Res Rev. 2022 Sep 12;14:319-326. doi: 10.2147/ORR.S381694. eCollection 2022. Orthop Res Rev. 2022. PMID: 36118013 Free PMC article.
-
Nonunion After Using Procedure-Specific Instrumentations for Ulnar Shortening Osteotomy.Arch Bone Jt Surg. 2023;11(11):677-683. doi: 10.22038/ABJS.2023.73837.3418. Arch Bone Jt Surg. 2023. PMID: 38058964 Free PMC article.
-
A Muscle Energy Techniques-Based Physiotherapeutic Intervention Protocol for Managing Nightstick Fracture: A Case Report.Cureus. 2024 Jan 31;16(1):e53353. doi: 10.7759/cureus.53353. eCollection 2024 Jan. Cureus. 2024. PMID: 38435862 Free PMC article.
-
Discovery of Posterior Oblique Ligament (POL) within the Distal Forearm Cruciate Complex (DFCC).Arch Bone Jt Surg. 2025;13(3):134-137. doi: 10.22038/ABJS.2025.85035.3872. Arch Bone Jt Surg. 2025. PMID: 40151584 Free PMC article.
-
Arthrex Mini Tightrope Fixation for Chronic Distal Radioulnar Joint Instability.Tech Hand Up Extrem Surg. 2023 Dec 1;27(4):243-248. doi: 10.1097/BTH.0000000000000446. Tech Hand Up Extrem Surg. 2023. PMID: 37490566 Free PMC article.
References
-
- Carr LW, Adams B. Chronic distal radioulnar joint instability. Hand Clin. 2020;36(4):443–453. - PubMed
-
- Poppler LH, Moran SL. Acute distal radioulnar joint instability: Evaluation and treatment. Hand Clin. 2020;36(4):429–441. - PubMed
-
- Rodriguez Merchan EC, De la Corte H. Injuries of the distal radioulnar joint. Contemp Orthop . 1994;29(3):193–200. - PubMed
-
- Ekenstam FA, Hagert CG. Anatomical studies on the geometry and stability of the distal radio ulnar joint. Scand J Plast Reconstr Surg. 1985;19(1):17–25. - PubMed
-
- af Ekenstam FW, Palmer AK, Glisson RR. The load on the radius and ulna in different positions of the wrist and forearm A cadaver study. Acta Orthop Scand. 1984;55(3):363–365. - PubMed
Publication types
LinkOut - more resources
Full Text Sources