

This is a preprint.
Immune phenotypes that predict COVID-19 severity
- PMID: 35291290
- PMCID: PMC8923110
- DOI: 10.21203/rs.3.rs-1378671/v1
Immune phenotypes that predict COVID-19 severity
Update in
-
Immune phenotypes that are associated with subsequent COVID-19 severity inferred from post-recovery samples.Nat Commun. 2022 Nov 25;13(1):7255. doi: 10.1038/s41467-022-34638-2. Nat Commun. 2022. PMID: 36433939 Free PMC article.
Abstract
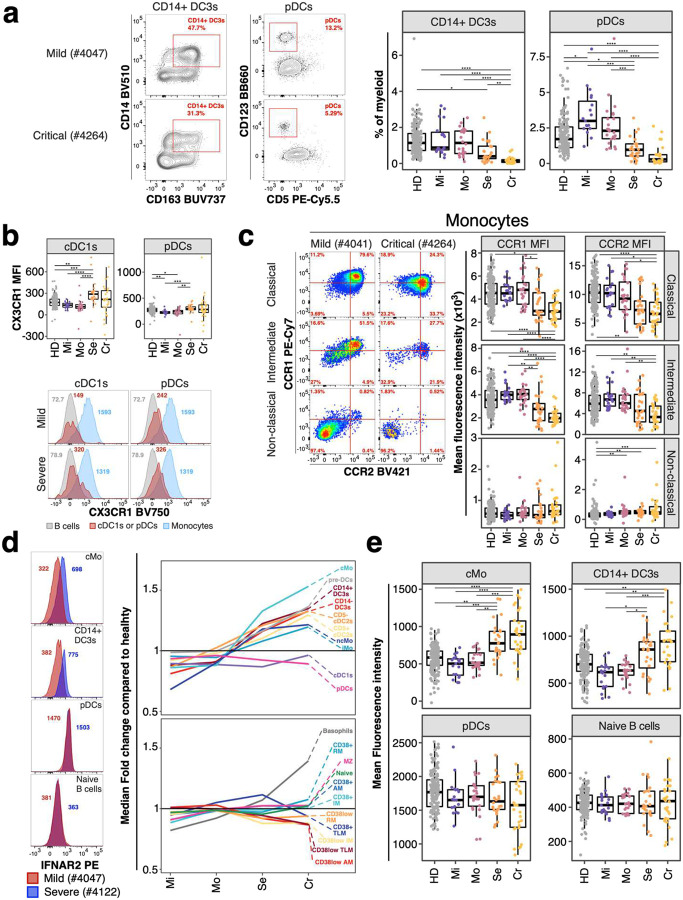
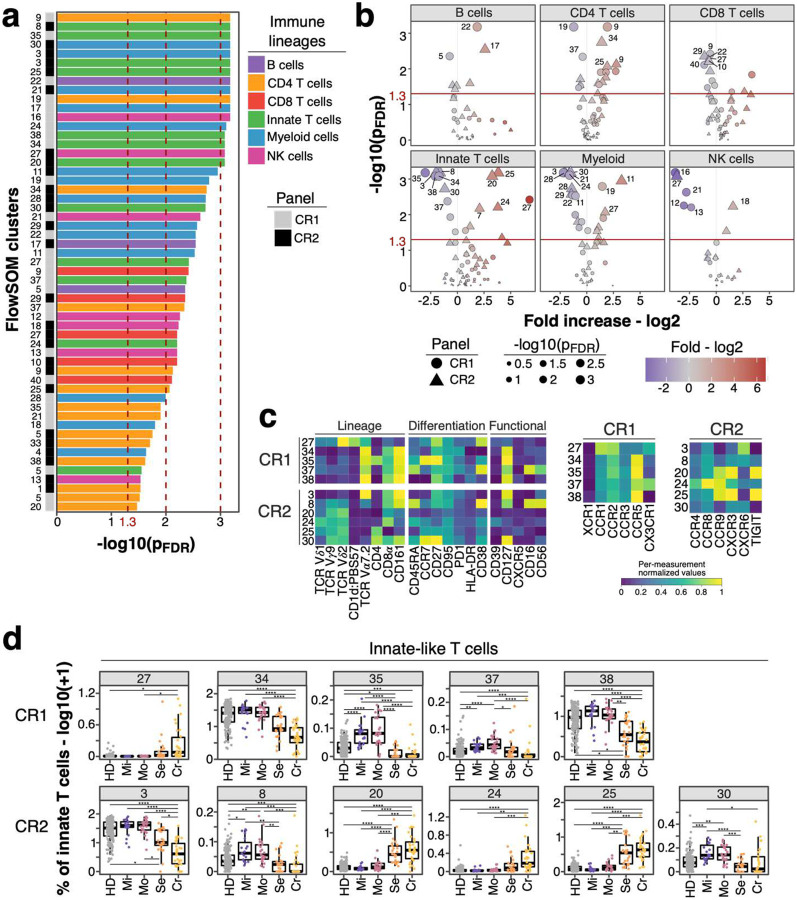
Severe COVID-19 causes profound immune perturbations, but pre-infection immune signatures contributing to severe COVID-19 remain unknown. Genome-wide association studies (GWAS) identified strong associations between severe disease and several chemokine receptors and molecules from the type I interferon pathway. Here, we define immune signatures associated with severe COVID-19 using high-dimensional flow cytometry. We measured the peripheral immune system from individuals who recovered from mild, moderate, severe or critical COVID-19 and focused only on those immune signatures returning to steady-state. Individuals that suffered from severe COVID-19 showed reduced frequencies of T cell, MAIT cell and dendritic cell (DCs) subsets and altered chemokine receptor expression on several subsets, such as reduced levels of CCR1 and CCR2 on monocyte subsets. Furthermore, we found reduced frequencies of type I interferon-producing plasmacytoid DCs and altered IFNAR2 expression on several myeloid cells in individuals recovered from severe COVID-19. Thus, these data identify potential immune mechanisms contributing to severe COVID-19.
Conflict of interest statement
Competing interests
None
Figures







References
-
- Pairo-Castineira E., Clohisey S., Klaric L., Bretherick A. D., Rawlik K., Pasko D., Walker S., Parkinson N., Fourman M. H., Russell C. D., Furniss J., Richmond A., Gountouna E., Wrobel N., Harrison D., Wang B., Wu Y., Meynert A., Griffiths F., Oosthuyzen W., Kousathanas A., Moutsianas L., Yang Z., Zhai R., Zheng C., Grimes G., Beale R., Millar J., Shih B., Keating S., Zechner M., Haley C., Porteous D. J., Hayward C., Yang J., Knight J., Summers C., Shankar-Hari M., Klenerman P., Turtle L., Ho A., Moore S. C., Hinds C., Horby P., Nichol A., Maslove D., Ling L., McAuley D., Montgomery H., Walsh T., Pereira A. C., Renieri A., Gen O. I., Investigators I. C., Initiative C.-H. G., andMe I., Investigators B., Gen C. I., Shen X., Ponting C. P., Fawkes A., Tenesa A., Caulfield M., Scott R., Rowan K., Murphy L., Openshaw P. J. M., Semple M. G., Law A., Vitart V., Wilson J. F., Baillie J. K., Genetic mechanisms of critical illness in COVID-19. Nature 591, 92–98 (2021). - PubMed
-
- Roederer M., Quaye L., Mangino M., Beddall M. H., Mahnke Y., Chattopadhyay P., Tosi I., Napolitano L., Terranova Barberio M., Menni C., Villanova F., Di Meglio P., Spector T. D., Nestle F. O., The genetic architecture of the human immune system: a bioresource for autoimmunity and disease pathogenesis. Cell 161, 387–403 (2015). - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
