

This is a preprint.
Sociodemographic Differences in Population-Level Immunosenescence in Older Age
- PMID: 35291293
- PMCID: PMC8923107
- DOI: 10.1101/2022.03.05.22271952
Sociodemographic Differences in Population-Level Immunosenescence in Older Age
Update in
-
Socioeconomic and race/ethnic differences in immunosenescence: Evidence from the Health and Retirement Study.Brain Behav Immun. 2023 Jan;107:361-368. doi: 10.1016/j.bbi.2022.10.019. Epub 2022 Nov 5. Brain Behav Immun. 2023. PMID: 36347419 Free PMC article.
Abstract
Background: The COVID-19 pandemic has highlighted the urgent need to understand variation in immunosenescence at the population-level. Thus far, population patterns of immunosenescence are not well described.
Methods: We characterized measures of immunosenescence from newly released venous blood data from the nationally representative U.S Health and Retirement Study (HRS) of individuals ages 56 years and older.
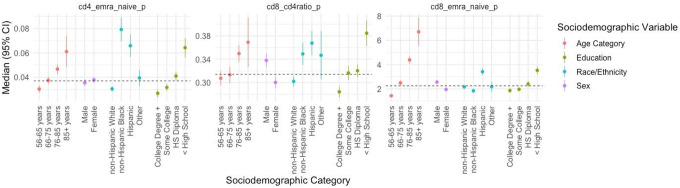
Findings: Median values of the CD8+:CD4+, EMRA:Nave CD4+ and EMRA:Nave CD8+ ratios were higher among older participants and were lower in those with additional educational attainment. Generally, minoritized race and ethnic groups had immune markers suggestive of a more aged immune profile: Hispanics had a CD8+:CD4+ median value of 0.37 (95% CI: 0.35, 0.39) compared to 0.30 in Whites (95% CI: 0.29, 0.31). Blacks had the highest median value of the EMRA:Nave CD4+ ratio (0.08; 95% CI: 0.07, 0.09) compared to Whites (0.03; 95% CI: 0.028, 0.033). In regression analyses, race/ethnicity and education were associated with large differences in the immune ratio measures after adjustment for age and sex. For example, each additional level of education was associated with roughly an additional decade of immunological age, and the racial/ethnic differences were associated with two to four decades of additional immunological age.
Interpretation: Our study provides novel insights into population variation in immunosenescence. This has implications for both risk of age-related disease and vulnerability to novel pathogens (e.g., SARS-CoV-2).
Funding: This study was partially funded by the U.S. National Institutes of Health, National Institute on Aging R00AG062749. AEA and GAN acknowledge support from the National Institutes of Health, National Institute on Aging R01AG075719. JBD acknowledges support from the Leverhulme Trust (Centre Grant) and the European Research Council grant ERC-2021-CoG-101002587.
Research in context: Evidence before this study: Alterations in immunity with chronological aging have been consistently demonstrated across human populations. Some of the hallmark changes in adaptive immunity associated with aging, termed immunosenescence, include a decrease in nave T-cells, an increase in terminal effector memory cells, and an inverted CD8:CD4 T cell ratio. Several studies have shown that social and psychosocial exposures can alter aspects of immunity and lead to increased susceptibility to infectious diseases.Add value of this study: While chronological age is known to impact immunosenescence, there are no studies examining whether social and demographic factors independently impact immunosenescence. This is important because immunosenescence has been associated with greater susceptibility to disease and lower immune response to vaccination. Identifying social and demographic variability in immunosenescence could help inform risk and surveillance efforts for preventing disease in older age. To our knowledge, we present one of the first large-scale population-based investigations of the social and demographic patterns of immunosenescence among individuals ages 50 and older living in the US. We found differences in the measures of immunosenescence by age, sex, race/ethnicity, and education, though the magnitude of these differences varied across immune measures and sociodemographic subgroup. Those occupying more disadvantaged societal positions (i.e., minoritized race and ethnic groups and individuals with lower educational attainment) experience greater levels of immunosenescence compared to those in less disadvantaged positions. Of note, the magnitude of effect of sociodemographic factors was larger than chronological age for many of the associations.Implications for practice or policy and future research: The COVID-19 pandemic has highlighted the need to better understand variation in adaptive and innate immunity at the population-level. While chronological age has traditionally been thought of as the primary driver of immunological aging, the magnitude of differences we observed by sociodemographic factors suggests an important role for the social environment in the aging human immune system.
Conflict of interest statement
Figures


Similar articles
-
Socioeconomic and race/ethnic differences in immunosenescence: Evidence from the Health and Retirement Study.Brain Behav Immun. 2023 Jan;107:361-368. doi: 10.1016/j.bbi.2022.10.019. Epub 2022 Nov 5. Brain Behav Immun. 2023. PMID: 36347419 Free PMC article.
-
Evaluation of T-cell aging-related immune phenotypes in the context of biological aging and multimorbidity in the Health and Retirement Study.Immun Ageing. 2022 Jul 20;19(1):33. doi: 10.1186/s12979-022-00290-z. Immun Ageing. 2022. PMID: 35858901 Free PMC article.
-
Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project.Res Rep Health Eff Inst. 2021 Sep;2021(208):1-127. Res Rep Health Eff Inst. 2021. PMID: 36106702 Free PMC article.
-
Impact of summer programmes on the outcomes of disadvantaged or 'at risk' young people: A systematic review.Campbell Syst Rev. 2024 Jun 13;20(2):e1406. doi: 10.1002/cl2.1406. eCollection 2024 Jun. Campbell Syst Rev. 2024. PMID: 38873396 Free PMC article. Review.
-
Immunosenescence: Implications for response to infection and vaccination in older people.Maturitas. 2015 Sep;82(1):50-5. doi: 10.1016/j.maturitas.2015.05.004. Epub 2015 May 18. Maturitas. 2015. PMID: 26044074 Review.
References
-
- Olsson J, Wikby A, Johansson B, Löfgren S, Nilsson B-O, Ferguson FG. Age-related change in peripheral blood T-lymphocyte subpopulations and cytomegalovirus infection in the very old: the Swedish longitudinal OCTO immune study. Mechanisms of ageing and development 2001; 121(1–3): 187–201. - PubMed
-
- Pawelec G, Koch S, Franceschi C, Wikby A. Human immunosenescence: does it have an infectious component? Annals of the New York Academy of Sciences 2006; 1067(1): 56–65. - PubMed
-
- Gkrania-Klotsas E, Langenberg C, Sharp SJ, Luben R, Khaw K-T, Wareham NJ. Seropositivity and higher immunoglobulin G antibody levels against cytomegalovirus are associated with mortality in the population-based European prospective investigation of cancer–Norfolk Cohort. Clinical infectious diseases 2013; 56(10): 1421–7. - PMC - PubMed
-
- Stassen FR, Vega-Córdova X, Vliegen I, Bruggeman CA. Immune activation following cytomegalovirus infection: more important than direct viral effects in cardiovascular disease? Journal of clinical virology 2006; 35(3): 349–53. - PubMed
-
- Grubeck-Loebenstein B, Della Bella S, Iorio AM, Michel J-P, Pawelec G, Solana R. Immunosenescence and vaccine failure in the elderly. Aging clinical and experimental research 2009; 21(3): 201–9. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous