

C reactive protein flare predicts response to checkpoint inhibitor treatment in non-small cell lung cancer
- PMID: 35292517
- PMCID: PMC8928397
- DOI: 10.1136/jitc-2021-004024
C reactive protein flare predicts response to checkpoint inhibitor treatment in non-small cell lung cancer
Abstract
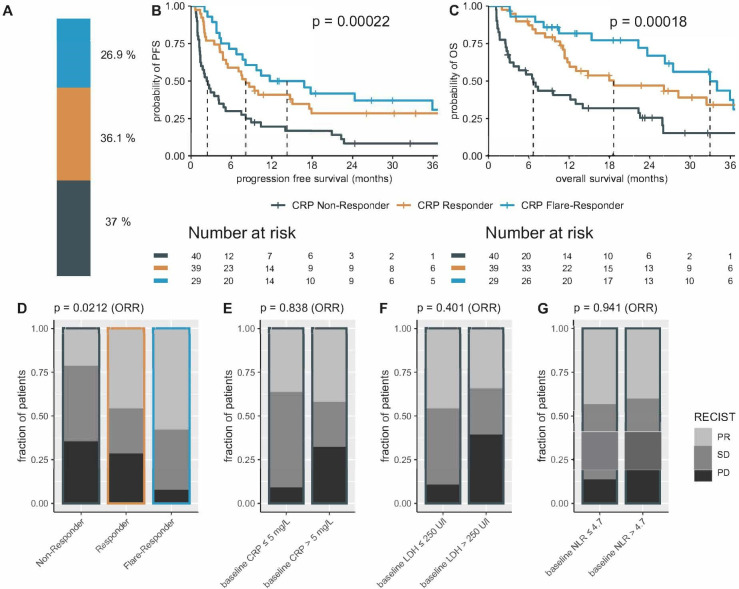
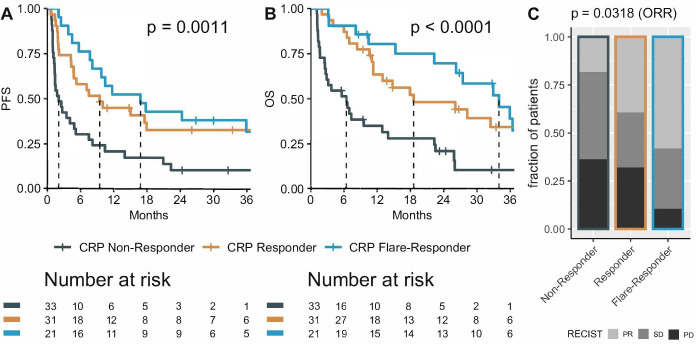
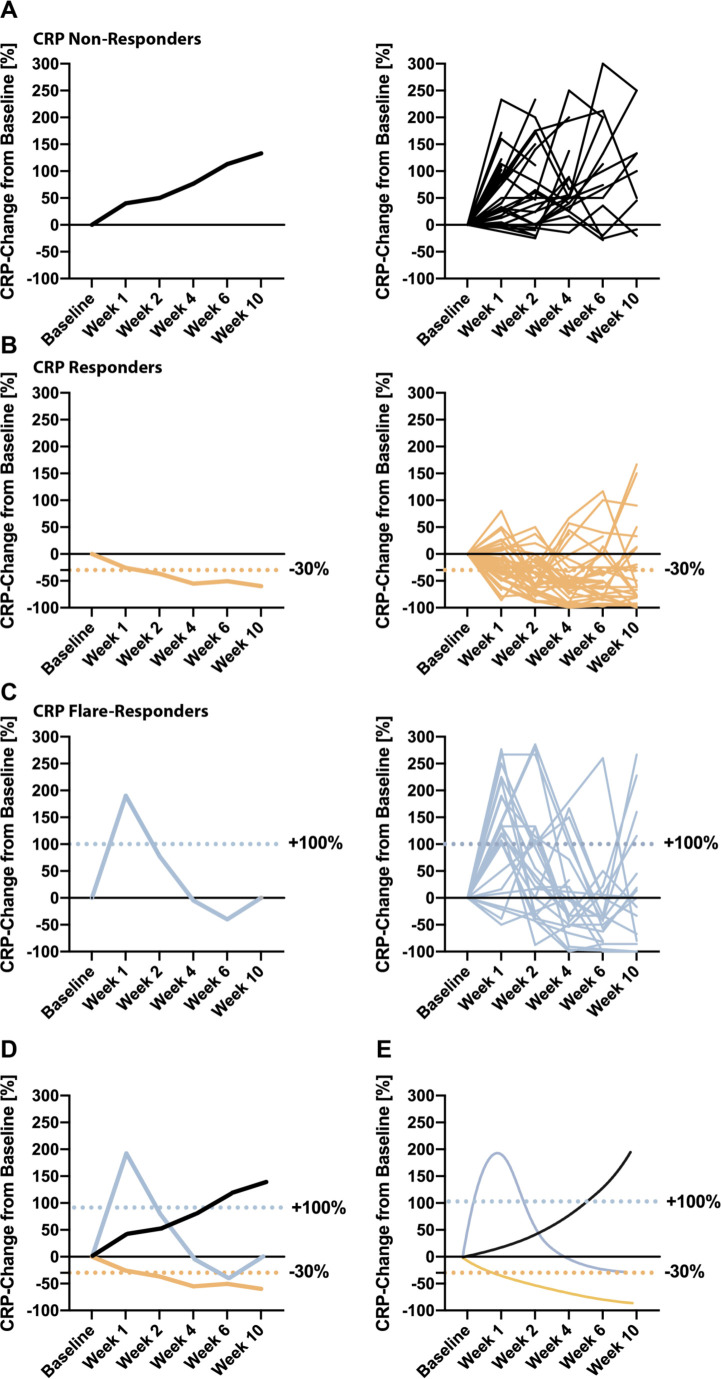
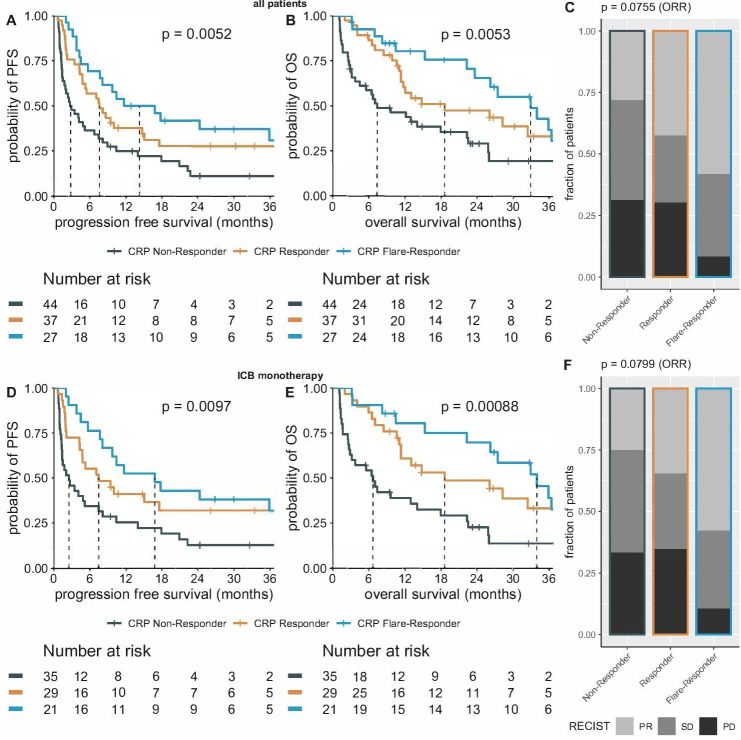
Biomarkers for predicting response to anti-programmed death-1 (PD-1) immune checkpoint blockade (ICB) in non-small cell lung cancer (NSCLC) remain in demand. Since anti-tumor immune activation is a process, early dynamic changes of the acute-phase reactant C reactive protein (CRP) may serve as a predictive on-treatment biomarker. In a retrospective (N=105) and prospective (N=108) ICB-treated NSCLC cohort, early CRP kinetics were stratified after the start of immunotherapy until weeks 4, 6, and 12 as follows: an early doubling of baseline CRP followed by a drop below baseline (CRP flare-responder), a drop of at least 30% below baseline without prior flare (CRP responders), or those who remained as CRP non-responders. In our study, we observed characteristic longitudinal changes of serum CRP concentration after the initiation of ICB. In the prospective cohort, N=40 patients were defined as CRP non-responders, N=39 as CRP responders, and N=29 as CRP flare-responders with a median progression-free survival (PFS) of 2.4, 8.1, and 14.3 months, respectively, and overall survival (OS) of 6.6, 18.6, and 32.9 months (both log-rank p<0.001). Of note, CRP flare-responses, characterized by a sharp on-treatment CRP increase in the first weeks after therapy initiation, followed by a decrease of CRP serum level below baseline, predict ICB response as early as 4 weeks after therapy initiation. Of note, early CRP kinetics showed no predictive value for chemoimmunotherapy or when steroids were administered concurrently. On-treatment CRP kinetics had a predictive value for both major histological NSCLC subtypes, adenocarcinoma and squamous cell carcinoma. The results were verified in an independent retrospective cohort of 105 patients. In conclusion, CRP flare predicted anti-PD-1 monotherapy response and survival in two independent cohorts including a total of 213 patients with NSCLC, regardless of histology. Due to its wide clinical availability, early CRP kinetics could become an easily determined, cost-efficient, and non-invasive biomarker to predict response to checkpoint inhibitors in NSCLC within the first month.
Keywords: biomarkers, tumor; immunotherapy; lung neoplasms.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous