

Cardiovascular imaging following perioperative myocardial infarction/injury
- PMID: 35292719
- PMCID: PMC8924205
- DOI: 10.1038/s41598-022-08261-6
Cardiovascular imaging following perioperative myocardial infarction/injury
Abstract
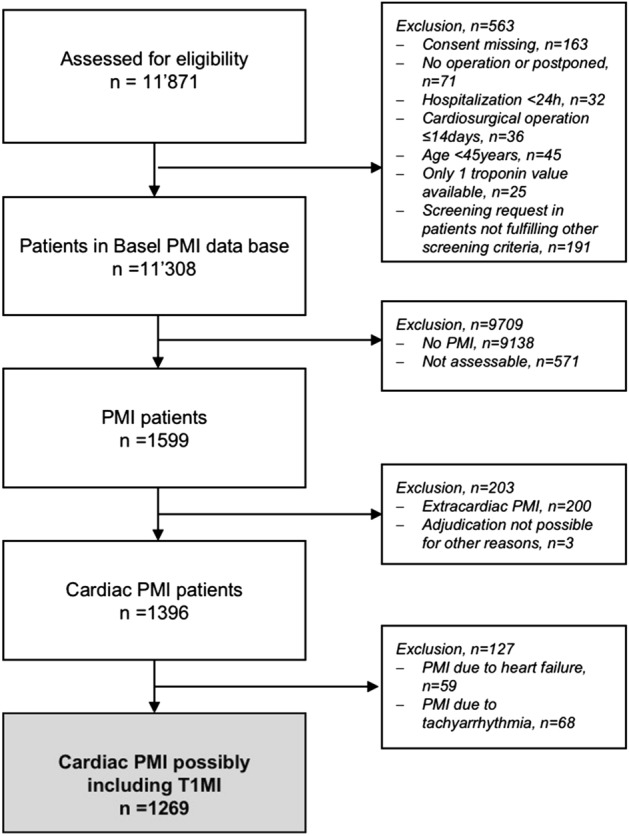
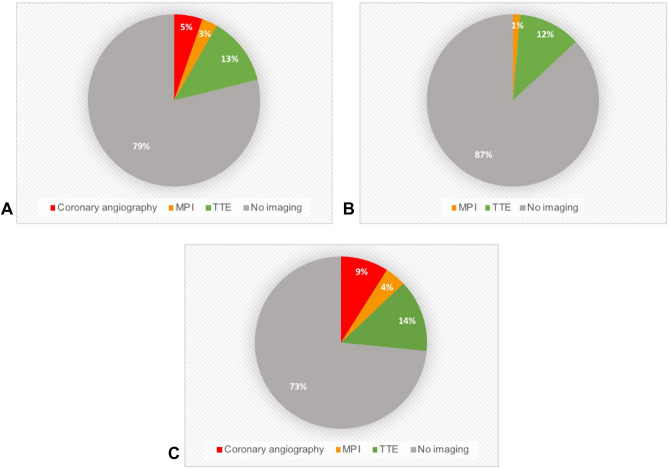
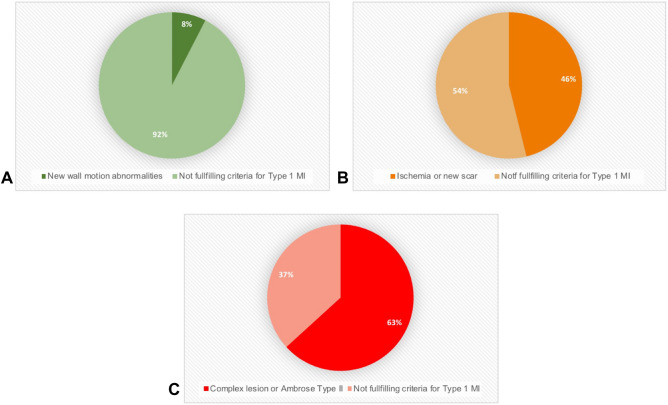
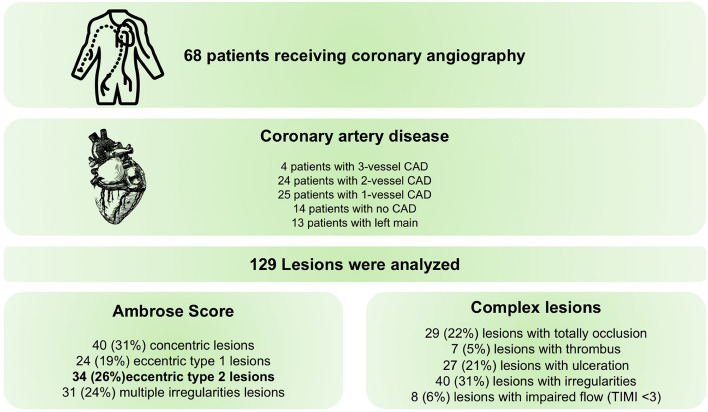
Patients developing perioperative myocardial infarction/injury (PMI) have a high mortality. PMI work-up and therapy remain poorly defined. This prospective multicenter study included high-risk patients undergoing major non-cardiac surgery within a systematic PMI screening and clinical response program. The frequency of cardiovascular imaging during PMI work-up and its yield for possible type 1 myocardial infarction (T1MI) was assessed. Automated PMI detection triggered evaluation by the treating physician/cardiologist, who determined selection/timing of cardiovascular imaging. T1M1 was considered with the presence of a new wall motion abnormality within 30 days in transthoracic echocardiography (TTE), a new scar or ischemia within 90 days in myocardial perfusion imaging (MPI), and Ambrose-Type II or complex lesions within 7 days of PMI in coronary angiography (CA). In patients with PMI, 21% (268/1269) underwent at least one cardiac imaging modality. TTE was used in 13% (163/1269), MPI in 3% (37/1269), and CA in 5% (68/1269). Cardiology consultation was associated with higher use of cardiovascular imaging (27% versus 13%). Signs indicative of T1MI were found in 8% of TTE, 46% of MPI, and 63% of CA. Most patients with PMI did not undergo any cardiovascular imaging within their PMI work-up. If performed, MPI and CA showed high yield for signs indicative of T1MI.Trial registration: https://clinicaltrials.gov/ct2/show/NCT02573532 .
© 2022. The Author(s).
Conflict of interest statement
Dr. Arslani has received a research grant from the Swiss Academy of Medical Sciences and the Bangerter Foundation (YTCR 09/19) and the Swiss National Science Foundation (P500PM_202963). Dr. Puelacher reports grants from PhD Educational Platform for Health Sciences, Roche Diagnostics and the University Hospital Basel during the conduct of the study. Dr. Gualandro has received research grants from FAPESP (Sao Paulo Research Foundation) for the submitted work, grants from the Swiss Heart Foundation and consulting honoraria from Roche, outside the submitted work. Dr. Mueller reports grants from the Swiss Heart Foundation and grants and non-financial support from several diagnostic companies during the conduct of the study, as well as grants, personal fees, and non-financial support from several diagnostic companies outside the submitted work. Dr. Kindler reports grants from the Forschungsfond Kantonsspital Aarau during the conduct of the study. Dr. Blum reports a grant from the Mach-Gaensslen Foundation outside the submitted work. All other authors report no conflicts of interest.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
