

The European MAPPYACTS Trial: Precision Medicine Program in Pediatric and Adolescent Patients with Recurrent Malignancies
- PMID: 35292802
- PMCID: PMC9394403
- DOI: 10.1158/2159-8290.CD-21-1136
The European MAPPYACTS Trial: Precision Medicine Program in Pediatric and Adolescent Patients with Recurrent Malignancies
Abstract
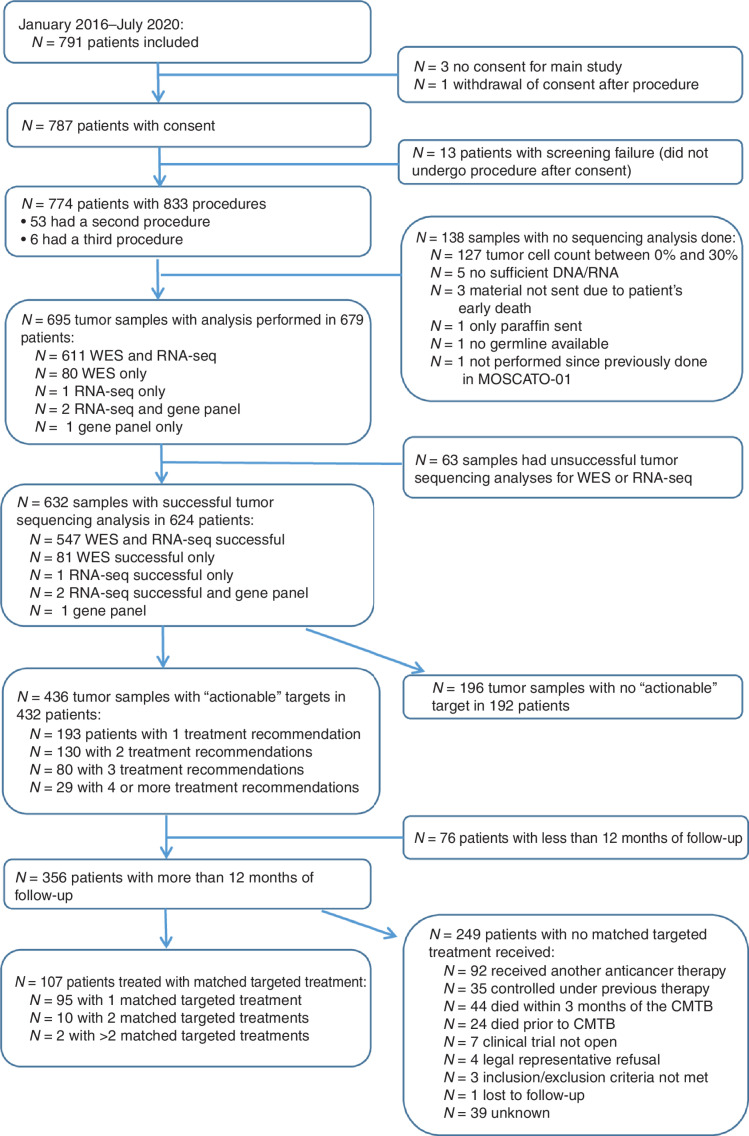
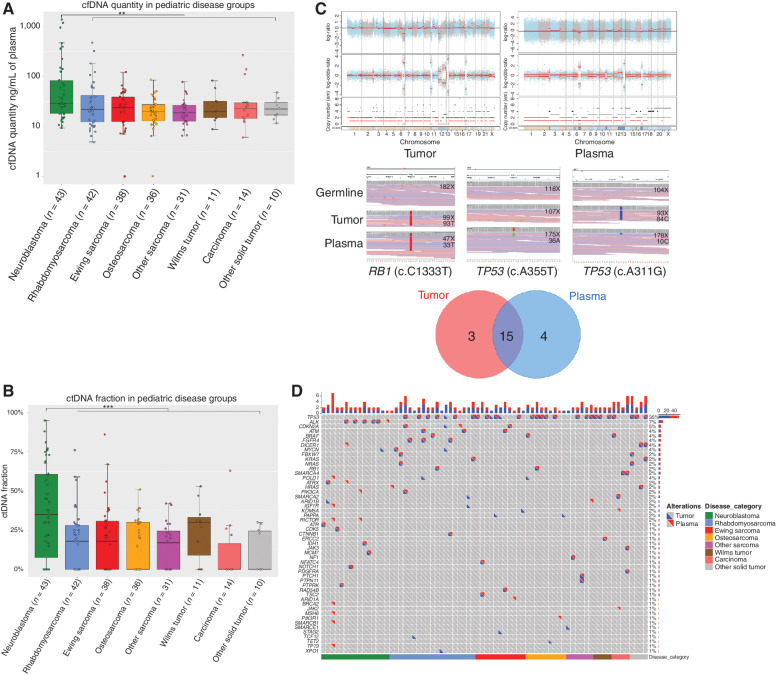
Abstract: MAPPYACTS (NCT02613962) is an international prospective precision medicine trial aiming to define tumor molecular profiles in pediatric patients with recurrent/refractory malignancies in order to suggest the most adapted salvage treatment. From February 2016 to July 2020, 787 patients were included in France, Italy, Ireland, and Spain. At least one genetic alteration leading to a targeted treatment suggestion was identified in 436 patients (69%) with successful sequencing; 10% of these alterations were considered "ready for routine use." Of 356 patients with follow-up beyond 12 months, 107 (30%) received one or more matched targeted therapies-56% of them within early clinical trials-mainly in the AcSé-ESMART platform trial (NCT02813135). Overall, matched treatment resulted in a 17% objective response rate, and of those patients with ready for routine use alterations, it was 38%. In patients with extracerebral tumors, 76% of actionable alterations detected in tumor tissue were also identified in circulating cell-free DNA (cfDNA).
Significance: MAPPYACTS underlines the feasibility of molecular profiling at cancer recurrence in children on a multicenter, international level and demonstrates benefit for patients with selected key drivers. The use of cfDNA deserves validation in prospective studies. Our study highlights the need for innovative therapeutic proof-of-concept trials that address the underlying cancer complexity. This article is highlighted in the In This Issue feature, p. 1171.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
- Cancer Discov. 12:1171.
- Cancer Discov. 12:1171.
References
-
- Gatta G, Botta L, Rossi S, Aareleid T, Bielska-Lasota M, Clavel J, et al. Childhood cancer survival in Europe 1999–2007: results of EUROCARE-5—a population-based study. Lancet Oncol 2014;15:35–47. - PubMed
-
- Massard C, Michiels S, Ferté C, Le Deley MC, Lacroix L, Hollebecque A, et al. High-throughput genomics and clinical outcome in hard-to-treat advanced cancers: results of the MOSCATO 01 trial. Cancer Discov 2017;7:586–95. - PubMed
-
- Le Tourneau C, Delord JP, Gonçalves A, Gavoille C, Dubot C, Isambert N, et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol 2015;16:1324–34. - PubMed
-
- Trédan O, Wang Q, Pissaloux D, Cassier P, de la Fouchardière A, Fayette J, et al. Molecular screening program to select molecular-based recommended therapies for metastatic cancer patients: analysis from the ProfiLER trial. Ann Oncol 2019;30:757–65. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
